IgG4 elevation dilemma at the crossroads of helminth infection and IgG4-related disease: insights from a case report of pediatric paragonimiasis with persistent pericardial effusion.
{"title":"IgG4 elevation dilemma at the crossroads of helminth infection and IgG4-related disease: insights from a case report of pediatric paragonimiasis with persistent pericardial effusion.","authors":"Zhan Zhang, Hua Zhou, Feng Fang, Guo Ai","doi":"10.21037/tp-2024-531","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is a systemic fibroinflammatory disorder defined by elevated serum IgG4, tissue IgG4+ plasma cell infiltration, and multi-organ involvement. Paradoxically, helminth infections may also trigger IgG4 elevation through Th2-polarized immune responses, creating diagnostic ambiguity when overlapping features occur. Critically, no studies have addressed whether IgG4-RD with helminthiasis can coexist in children or how to differentiate them when histopathology is unavailable.</p><p><strong>Case description: </strong>A 10-year-old boy with confirmed pulmonary paragonimiasis developed refractory pericardial effusion and markedly elevated IgG4 [11 g/L, 8.1× upper limit of normal (ULN)]. Despite five courses of praziquantel (75 mg/kg/day), effusions persisted for 8 weeks. Subsequent glucocorticoids (methylprednisolone 2 mg/kg/day) achieved rapid clinical resolution, though lacked histopathology IgG4-RD hallmarks. Longitudinal monitoring revealed a dynamic IgG4 decline (from 11 to 5.25 g/L) post-methylprednisolone therapy. However, residual IgG4 elevation (5.25 g/L, >3× ULN) and absent histopathological features of IgG4-RD left the diagnosis unresolved. Therapeutic monitoring revealed normalized eosinophils and imaging improvement, yet persistent IgG4 suggested potential immune dysregulation beyond parasitic clearance.</p><p><strong>Conclusions: </strong>This case highlights a critical diagnostic dilemma: IgG4 elevation in parasitic infections may mimic or coexist with IgG4-RD. The rapid glucocorticoid response argues against simple parasitic infections, yet incomplete IgG4 normalization post-treatment leaves coexistence unresolved. Clinicians must weigh these possibilities when anti-helminthic therapy fails, particularly when histopathology is absent. Prospective studies should define pediatric-specific IgG4 thresholds to disentangle infection from autoimmunity.</p>","PeriodicalId":23294,"journal":{"name":"Translational pediatrics","volume":"14 6","pages":"1362-1369"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12268758/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tp-2024-531","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is a systemic fibroinflammatory disorder defined by elevated serum IgG4, tissue IgG4+ plasma cell infiltration, and multi-organ involvement. Paradoxically, helminth infections may also trigger IgG4 elevation through Th2-polarized immune responses, creating diagnostic ambiguity when overlapping features occur. Critically, no studies have addressed whether IgG4-RD with helminthiasis can coexist in children or how to differentiate them when histopathology is unavailable.
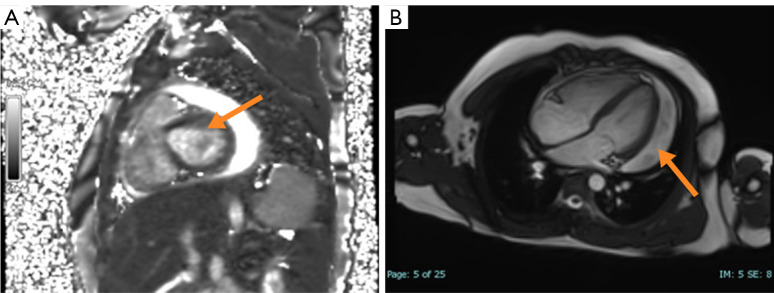
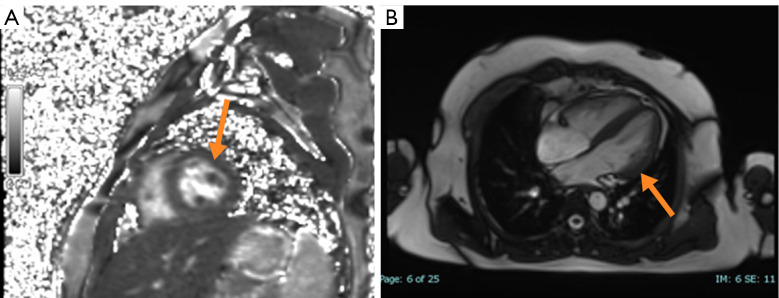
Case description: A 10-year-old boy with confirmed pulmonary paragonimiasis developed refractory pericardial effusion and markedly elevated IgG4 [11 g/L, 8.1× upper limit of normal (ULN)]. Despite five courses of praziquantel (75 mg/kg/day), effusions persisted for 8 weeks. Subsequent glucocorticoids (methylprednisolone 2 mg/kg/day) achieved rapid clinical resolution, though lacked histopathology IgG4-RD hallmarks. Longitudinal monitoring revealed a dynamic IgG4 decline (from 11 to 5.25 g/L) post-methylprednisolone therapy. However, residual IgG4 elevation (5.25 g/L, >3× ULN) and absent histopathological features of IgG4-RD left the diagnosis unresolved. Therapeutic monitoring revealed normalized eosinophils and imaging improvement, yet persistent IgG4 suggested potential immune dysregulation beyond parasitic clearance.
Conclusions: This case highlights a critical diagnostic dilemma: IgG4 elevation in parasitic infections may mimic or coexist with IgG4-RD. The rapid glucocorticoid response argues against simple parasitic infections, yet incomplete IgG4 normalization post-treatment leaves coexistence unresolved. Clinicians must weigh these possibilities when anti-helminthic therapy fails, particularly when histopathology is absent. Prospective studies should define pediatric-specific IgG4 thresholds to disentangle infection from autoimmunity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


