Clara Hjalmarsson, Tanvee Thakur, Göran Rådegran, Erik Björklund, Håkan Wåhlander, Magnus Nisell, Joanna-Maria Papageorgiou, Stefan Söderberg, Dominik Lautsch, Barbro Kjellström
{"title":"Risk Assessment Models and Event-Free Survival in Pulmonary Arterial Hypertension.","authors":"Clara Hjalmarsson, Tanvee Thakur, Göran Rådegran, Erik Björklund, Håkan Wåhlander, Magnus Nisell, Joanna-Maria Papageorgiou, Stefan Söderberg, Dominik Lautsch, Barbro Kjellström","doi":"10.1002/pul2.70132","DOIUrl":null,"url":null,"abstract":"<p><p>Evidence on the predictive ability of risk assessment models for event-free survival (EFS) in patients with pulmonary arterial hypertension is scarce. We aimed to investigate the relationship between risk status at 6 months after diagnosis (6 M) and EFS, by three risk models: Multicomponent Improvement (MCI), ESC/ERS 4-Strata Risk (4SR), and noninvasive French PH Registry Score (FRS). Data collected in the Swedish PAH Registry 2008-2021 were used. The study population was risk-stratified at 6 M according to each model. Information on PAH-related hospitalization (HOSP) was collected from the National Patient Register. EFS was defined as survival without occurrence of: (1) HOSP; (2) initiation of parenteral prostacyclin therapy or dose increase ≥ 10%; (3) lung transplantation. The association between risk and EFS was evaluated by Kaplan-Meier estimates and Cox proportional models. The analysis included 411 incident patients, median age 66 y [50, 73]. Median survival time was 3.5 y [1.7; 5.4], and cumulative EFS was 55%. In a Cox proportional regression adjusted for age, eGFR, obesity, atrial fibrillation, and systemic hypertension, EFS was higher in patients who: (1) achieved two or three MCI criteria compared to one or no MCI criterion (HR 0.58; CI 0.39-0.84, <i>p</i> = 0.005); (2) were assessed as low, intermediate-low, or intermediate-high compared to high risk (HR 0.16; CI 0.09-0.28, <i>p</i> < 0.001); or (3) fulfilled one, two, or three low-risk FRS criteria, compared to no low-risk criterion (HR 0.29; CI 0.19-0.43, <i>p</i> < 0.001). Performing a risk assessment 6 months after diagnosis effectively predicts the likelihood of EFS in the studied population, highlighting its prognostic value.</p>","PeriodicalId":20927,"journal":{"name":"Pulmonary Circulation","volume":"15 3","pages":"e70132"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12272513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Circulation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pul2.70132","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
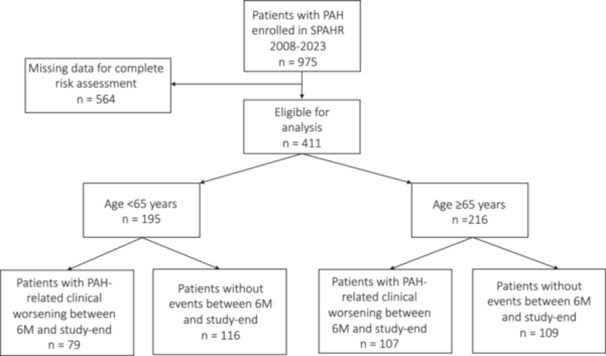
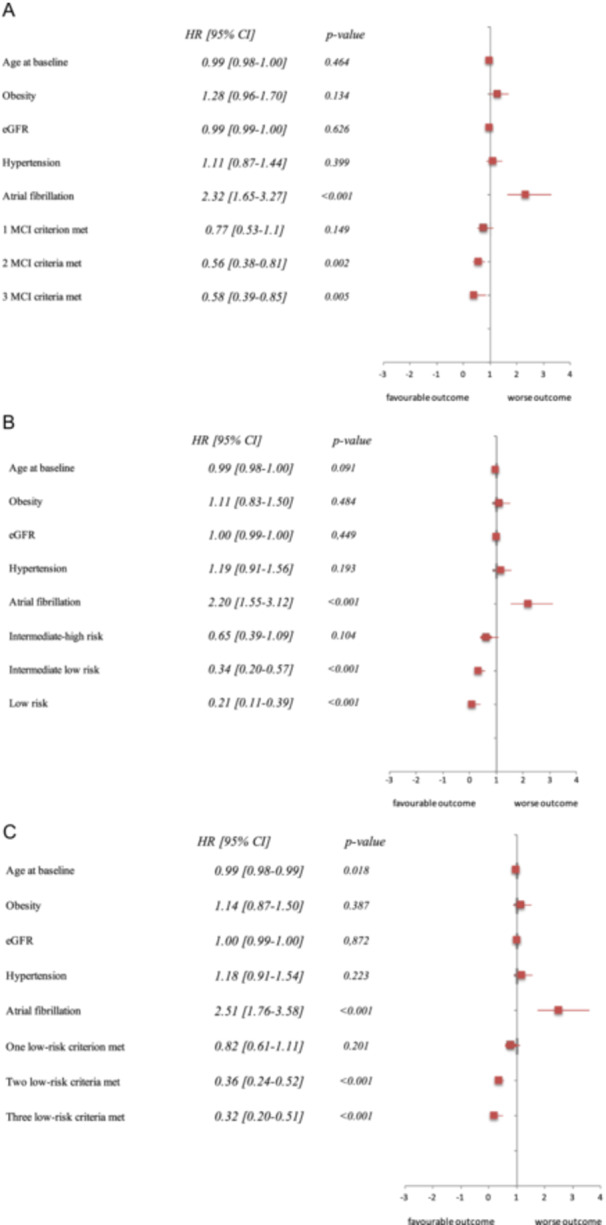
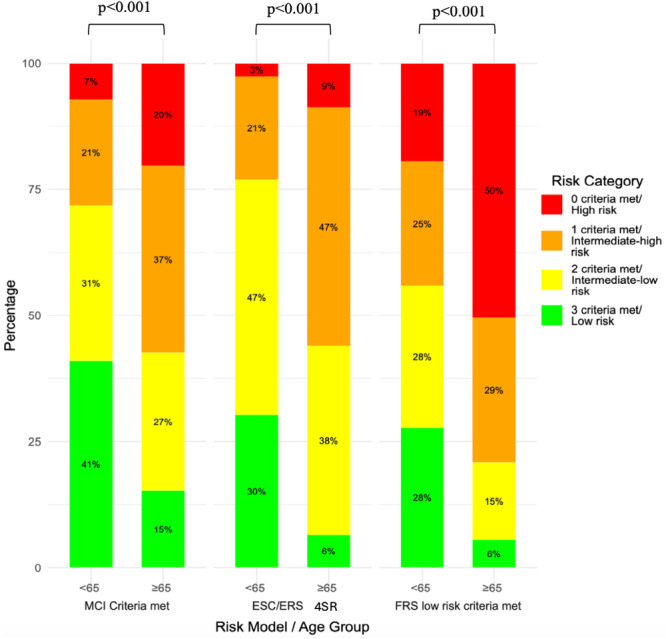
Evidence on the predictive ability of risk assessment models for event-free survival (EFS) in patients with pulmonary arterial hypertension is scarce. We aimed to investigate the relationship between risk status at 6 months after diagnosis (6 M) and EFS, by three risk models: Multicomponent Improvement (MCI), ESC/ERS 4-Strata Risk (4SR), and noninvasive French PH Registry Score (FRS). Data collected in the Swedish PAH Registry 2008-2021 were used. The study population was risk-stratified at 6 M according to each model. Information on PAH-related hospitalization (HOSP) was collected from the National Patient Register. EFS was defined as survival without occurrence of: (1) HOSP; (2) initiation of parenteral prostacyclin therapy or dose increase ≥ 10%; (3) lung transplantation. The association between risk and EFS was evaluated by Kaplan-Meier estimates and Cox proportional models. The analysis included 411 incident patients, median age 66 y [50, 73]. Median survival time was 3.5 y [1.7; 5.4], and cumulative EFS was 55%. In a Cox proportional regression adjusted for age, eGFR, obesity, atrial fibrillation, and systemic hypertension, EFS was higher in patients who: (1) achieved two or three MCI criteria compared to one or no MCI criterion (HR 0.58; CI 0.39-0.84, p = 0.005); (2) were assessed as low, intermediate-low, or intermediate-high compared to high risk (HR 0.16; CI 0.09-0.28, p < 0.001); or (3) fulfilled one, two, or three low-risk FRS criteria, compared to no low-risk criterion (HR 0.29; CI 0.19-0.43, p < 0.001). Performing a risk assessment 6 months after diagnosis effectively predicts the likelihood of EFS in the studied population, highlighting its prognostic value.
期刊介绍:
Pulmonary Circulation''s main goal is to encourage basic, translational, and clinical research by investigators, physician-scientists, and clinicans, in the hope of increasing survival rates for pulmonary hypertension and other pulmonary vascular diseases worldwide, and developing new therapeutic approaches for the diseases. Freely available online, Pulmonary Circulation allows diverse knowledge of research, techniques, and case studies to reach a wide readership of specialists in order to improve patient care and treatment outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


