Jean-Bonny Nsumbu, Jean-Robert Makulo, Trésor Mutombo Tshiswaka, Christian Kisoka Lusunsi, Charles Nlombi Mbendi
{"title":"Performance of APRI and FIB-4 Scores Compared to FibroScan: A Cross-Sectional Study in a Black Sub-Saharan African Population.","authors":"Jean-Bonny Nsumbu, Jean-Robert Makulo, Trésor Mutombo Tshiswaka, Christian Kisoka Lusunsi, Charles Nlombi Mbendi","doi":"10.2147/HMER.S533064","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aim: </strong>Several non-invasive tests are used to assess liver fibrosis and cirrhosis in patients with liver disease. However, most validation studies have not included populations in sub-Saharan Africa. This study aimed to evaluate the diagnostic performance of the APRI and FIB-4 scores in a Congolese cohort.</p><p><strong>Patients and methods: </strong>A cohort of patients in Kinshasa underwent FibroScan and laboratory testing to calculate APRI and FIB-4 scores. Pearson correlation, sensitivity, specificity, and ROC curve analyses were used to evaluate the performance of these non-invasive scores against FibroScan. Cirrhosis was defined as liver stiffness ≥14 kPa by FibroScan. Thresholds for APRI and FIB-4 scores predicting cirrhosis were set at ≥ 1.5 and ≥ 2.67, respectively.</p><p><strong>Results: </strong>The study included 316 patients (mean ± SD age: 48.1 ± 14.1 years; 60.8% male; 10.1% with diabetes; 37.1% obese; 14.2% with hepatitis B; 6.7% with hepatitis C; 25.6% with a history of alcohol use). The Pearson correlation between APRI and FibroScan was r = 0.210 (p < 0.001), while the correlation between FIB-4 and FibroScan was better (r = 0.478, p < 0.001). In subgroup analyses, FIB-4 correlated with FibroScan only among patients with alcohol use or hepatitis B or C, APRI only correlated with FibroScan in alcohol dependent patients. The sensitivity and specificity of APRI were 29.7% and 97.9% respectively, compared to 60.0% and 93.3% for FibroScan. The areas under the ROC curve were 0.8462 for APRI and 0.8312 for FIB-4, with thresholds lower than those reported in the literature: 0.422 for APRI and 1.285 for FIB-4, but these varied according to the subgroup.</p><p><strong>Conclusion: </strong>APRI and FIB-4 scores demonstrate high specificity but low sensitivity for diagnosing cirrhosis in this population. Their diagnostic performance is notably better in patients with alcohol-related liver disease or viral hepatitis, but poor among those with diabetes or obesity.</p>","PeriodicalId":12917,"journal":{"name":"Hepatic Medicine : Evidence and Research","volume":"17 ","pages":"27-37"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12275969/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatic Medicine : Evidence and Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/HMER.S533064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aim: Several non-invasive tests are used to assess liver fibrosis and cirrhosis in patients with liver disease. However, most validation studies have not included populations in sub-Saharan Africa. This study aimed to evaluate the diagnostic performance of the APRI and FIB-4 scores in a Congolese cohort.
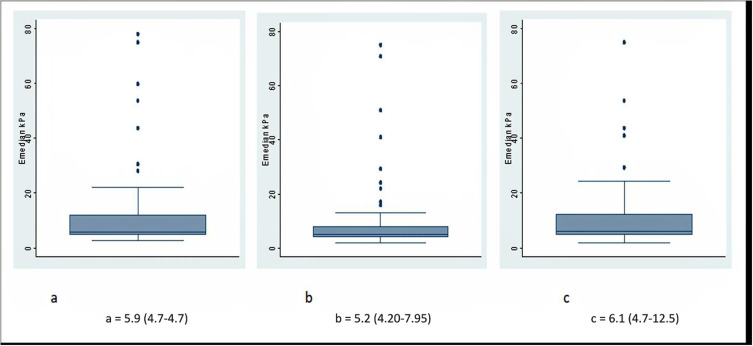
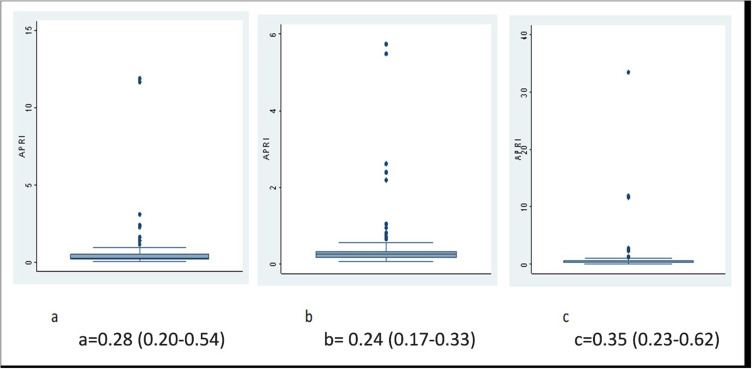
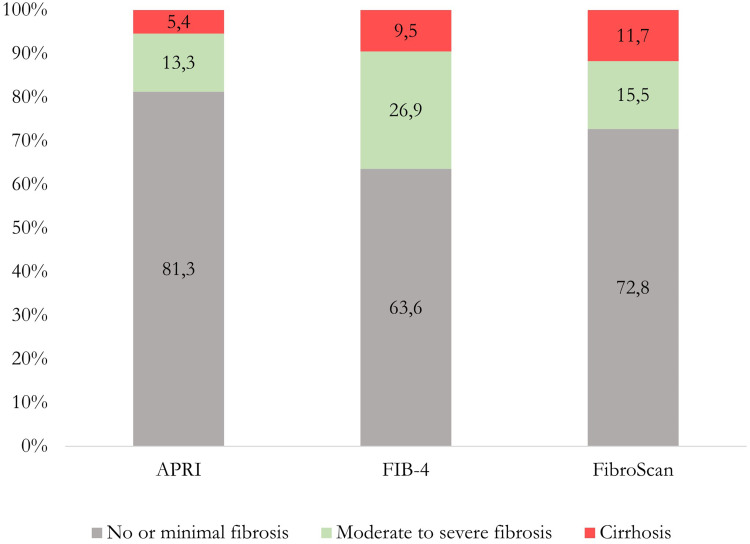
Patients and methods: A cohort of patients in Kinshasa underwent FibroScan and laboratory testing to calculate APRI and FIB-4 scores. Pearson correlation, sensitivity, specificity, and ROC curve analyses were used to evaluate the performance of these non-invasive scores against FibroScan. Cirrhosis was defined as liver stiffness ≥14 kPa by FibroScan. Thresholds for APRI and FIB-4 scores predicting cirrhosis were set at ≥ 1.5 and ≥ 2.67, respectively.
Results: The study included 316 patients (mean ± SD age: 48.1 ± 14.1 years; 60.8% male; 10.1% with diabetes; 37.1% obese; 14.2% with hepatitis B; 6.7% with hepatitis C; 25.6% with a history of alcohol use). The Pearson correlation between APRI and FibroScan was r = 0.210 (p < 0.001), while the correlation between FIB-4 and FibroScan was better (r = 0.478, p < 0.001). In subgroup analyses, FIB-4 correlated with FibroScan only among patients with alcohol use or hepatitis B or C, APRI only correlated with FibroScan in alcohol dependent patients. The sensitivity and specificity of APRI were 29.7% and 97.9% respectively, compared to 60.0% and 93.3% for FibroScan. The areas under the ROC curve were 0.8462 for APRI and 0.8312 for FIB-4, with thresholds lower than those reported in the literature: 0.422 for APRI and 1.285 for FIB-4, but these varied according to the subgroup.
Conclusion: APRI and FIB-4 scores demonstrate high specificity but low sensitivity for diagnosing cirrhosis in this population. Their diagnostic performance is notably better in patients with alcohol-related liver disease or viral hepatitis, but poor among those with diabetes or obesity.
期刊介绍:
Hepatic Medicine: Evidence and Research is an international, peer-reviewed, open access, online journal. Publishing original research, reports, editorials, reviews and commentaries on all aspects of adult and pediatric hepatology in the clinic and laboratory including the following topics: Pathology, pathophysiology of hepatic disease Investigation and treatment of hepatic disease Pharmacology of drugs used for the treatment of hepatic disease Although the main focus of the journal is to publish research and clinical results in humans; preclinical, animal and in vitro studies will be published where they will shed light on disease processes and potential new therapies. Issues of patient safety and quality of care will also be considered. As of 1st April 2019, Hepatic Medicine: Evidence and Research will no longer consider meta-analyses for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


