Isabella Chiardi, Laura Croce, Paolo Caccavale, Jacopo Bertini, Francesca Coperchini, Flavia Magri, Carlo Cappelli, Pierpaolo Trimboli, Mario Rotondi
{"title":"Establishing the Adequate Levothyroxine Dose After Total Thyroidectomy: A Systematic Review With Meta-analysis.","authors":"Isabella Chiardi, Laura Croce, Paolo Caccavale, Jacopo Bertini, Francesca Coperchini, Flavia Magri, Carlo Cappelli, Pierpaolo Trimboli, Mario Rotondi","doi":"10.1210/clinem/dgaf417","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Total thyroidectomy requires lifelong levothyroxine (LT4) therapy. Achieving optimal thyroid hormone replacement at the first postoperative follow-up might be harder than expected. Despite the various LT4 dose-choosing strategies tested, there is no consensus on the most effective approach to achieve early euthyroidism.</p><p><strong>Materials and methods: </strong>We performed a systematic review and meta-analysis, including studies published between 2000 and 2024 that reported the proportion of patients achieving euthyroidism at first follow-up after total thyroidectomy. Data from 11 studies comprising 2577 patients were analyzed. LT4 dosing strategies included fixed-dose, weight-based (dose/kg), and individualized algorithm-based methods. Meta-regression and subgroup analyses were used to explore sources of heterogeneity.</p><p><strong>Results: </strong>The pooled euthyroidism rate at first follow-up was 33.9%, with high heterogeneity across studies (I2 = 82.68%). No dosing strategy consistently outperformed others: dose/kg methods achieved 29% euthyroidism, while fixed or algorithm-based approaches achieved 40%, though without statistical significance. Meta-regression analysis did not identify any statistically significant predictor. No significant differences emerged between patients treated for benign or malignant thyroid diseases or between retrospective and prospective study designs.</p><p><strong>Conclusion: </strong>Only about one-third of patients achieve euthyroidism at first follow-up after thyroidectomy, regardless of LT4 dosing strategy. The current guidelines recommendation of applying a pro/kg dose may not be adequate, and even personalized algorithms yield inconsistent results. Future prospective studies are needed to refine individualized dosing protocols and identify additional factors influencing LT4 requirements.</p>","PeriodicalId":520805,"journal":{"name":"The Journal of clinical endocrinology and metabolism","volume":" ","pages":"3301-3308"},"PeriodicalIF":5.1000,"publicationDate":"2025-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527440/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of clinical endocrinology and metabolism","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/clinem/dgaf417","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Total thyroidectomy requires lifelong levothyroxine (LT4) therapy. Achieving optimal thyroid hormone replacement at the first postoperative follow-up might be harder than expected. Despite the various LT4 dose-choosing strategies tested, there is no consensus on the most effective approach to achieve early euthyroidism.
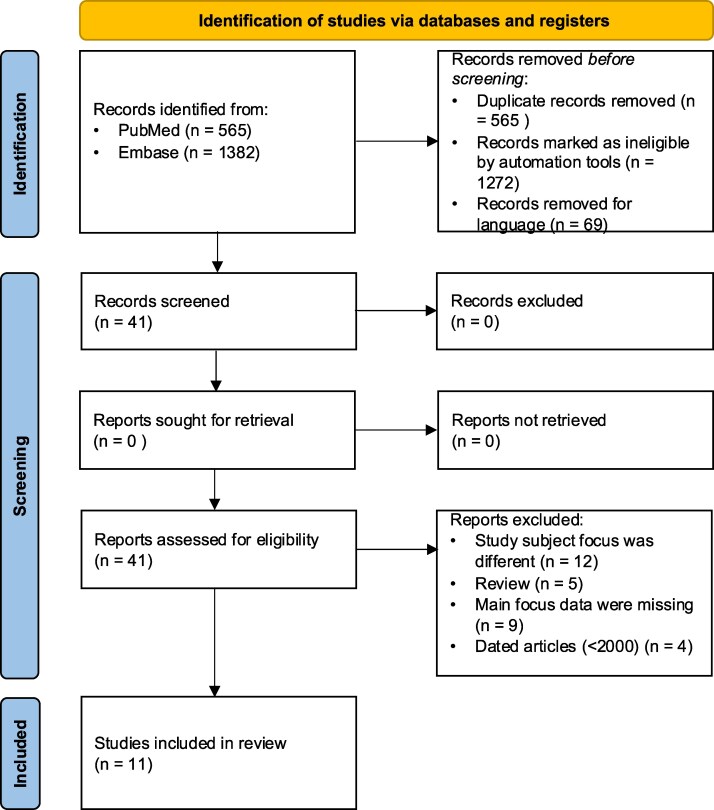
Materials and methods: We performed a systematic review and meta-analysis, including studies published between 2000 and 2024 that reported the proportion of patients achieving euthyroidism at first follow-up after total thyroidectomy. Data from 11 studies comprising 2577 patients were analyzed. LT4 dosing strategies included fixed-dose, weight-based (dose/kg), and individualized algorithm-based methods. Meta-regression and subgroup analyses were used to explore sources of heterogeneity.
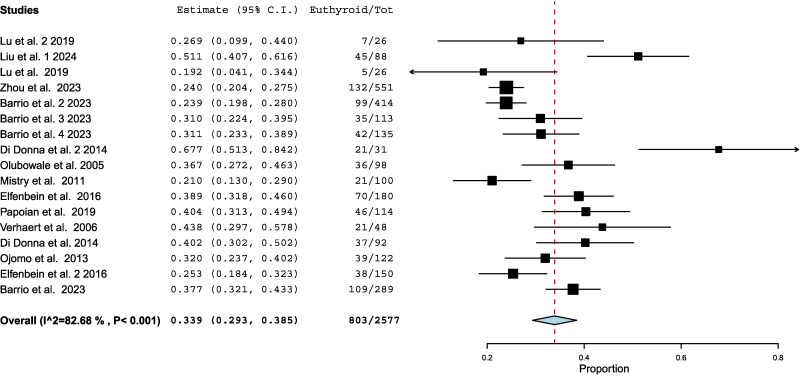
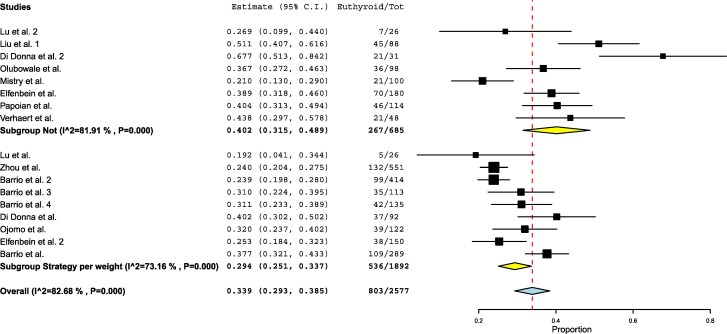
Results: The pooled euthyroidism rate at first follow-up was 33.9%, with high heterogeneity across studies (I2 = 82.68%). No dosing strategy consistently outperformed others: dose/kg methods achieved 29% euthyroidism, while fixed or algorithm-based approaches achieved 40%, though without statistical significance. Meta-regression analysis did not identify any statistically significant predictor. No significant differences emerged between patients treated for benign or malignant thyroid diseases or between retrospective and prospective study designs.
Conclusion: Only about one-third of patients achieve euthyroidism at first follow-up after thyroidectomy, regardless of LT4 dosing strategy. The current guidelines recommendation of applying a pro/kg dose may not be adequate, and even personalized algorithms yield inconsistent results. Future prospective studies are needed to refine individualized dosing protocols and identify additional factors influencing LT4 requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


