Robert Connor Chick, Samantha M Ruff, Ryan Heslin, Matthew R Porembka, Patricio M Polanco, Alex C Kim
{"title":"Risk of peritoneal metastasis following minimally invasive colectomy for locally advanced colon cancer: a systematic review and meta-analysis.","authors":"Robert Connor Chick, Samantha M Ruff, Ryan Heslin, Matthew R Porembka, Patricio M Polanco, Alex C Kim","doi":"10.1093/oncolo/oyaf218","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Locally advanced (T4) colon cancer is a significant risk factor for peritoneal metastasis (PM). Although laparoscopic colectomy (LC) is considered oncologically safe, the risk of PM in patients with T4 disease undergoing LC remains unclear. Prior systematic reviews demonstrated equivalent overall survival between LC and open colectomy (OC). However, comparison of LC and OC for peritoneal recurrence is lacking.</p><p><strong>Methods: </strong>A systematic review, conducted according to PRISMA guidelines, identified 247 abstracts, of which 46 full texts were reviewed. Studies including both LC and OC that reported peritoneal recurrence were included. Case reports and conference abstracts were excluded. Pooled effect size for proportion of, and hazard ratio (HR) for, peritoneal recurrence were calculated using a random-effects model with inverse variance weighting.</p><p><strong>Results: </strong>Nine studies met inclusion criteria. All were retrospective cohort studies; most considered \"conversion to open\" as laparoscopic procedures. Pooled odds ratio was 1.61 (P = .011, I2 = 0.62), and HR was 1.24 (P < .001, I2 = 0.10) for developing peritoneal metastases. Risk of bias was assessed as low or moderate for all studies. Quality of evidence was low.</p><p><strong>Conclusions: </strong>Laparoscopic colectomy is associated with an increased risk of peritoneal recurrence compared with open colectomy for T4 colon cancer. Although selection bias in these nonrandomized studies should favor laparoscopic surgery, LC was associated with an increased risk of peritoneal recurrence. LC should be approached with caution for cT4 colon cancer. Strategies to mitigate the risk of peritoneal recurrence in T4 colon cancer, such as neoadjuvant chemotherapy or adjuvant intraperitoneal chemotherapy, should be further explored in prospective studies.</p>","PeriodicalId":54686,"journal":{"name":"Oncologist","volume":" ","pages":""},"PeriodicalIF":4.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445660/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncologist","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/oncolo/oyaf218","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Locally advanced (T4) colon cancer is a significant risk factor for peritoneal metastasis (PM). Although laparoscopic colectomy (LC) is considered oncologically safe, the risk of PM in patients with T4 disease undergoing LC remains unclear. Prior systematic reviews demonstrated equivalent overall survival between LC and open colectomy (OC). However, comparison of LC and OC for peritoneal recurrence is lacking.
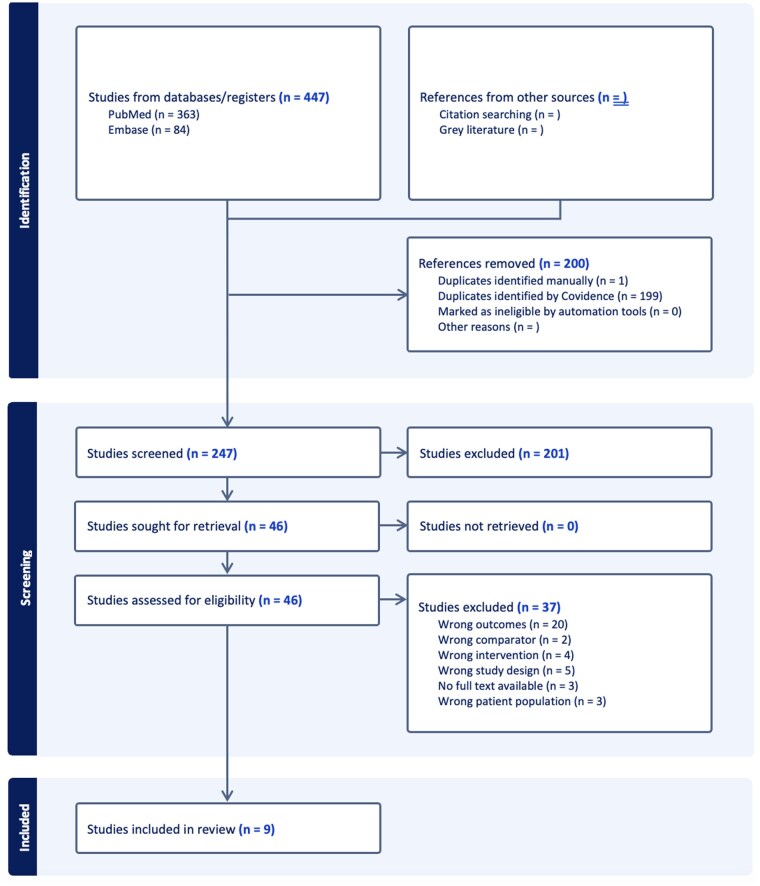
Methods: A systematic review, conducted according to PRISMA guidelines, identified 247 abstracts, of which 46 full texts were reviewed. Studies including both LC and OC that reported peritoneal recurrence were included. Case reports and conference abstracts were excluded. Pooled effect size for proportion of, and hazard ratio (HR) for, peritoneal recurrence were calculated using a random-effects model with inverse variance weighting.
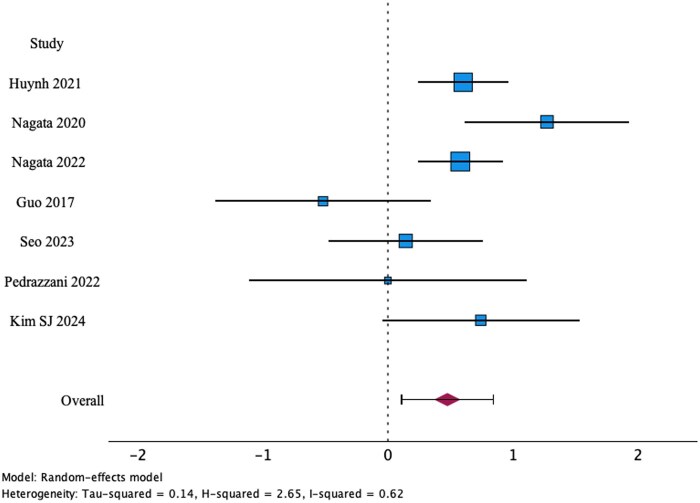
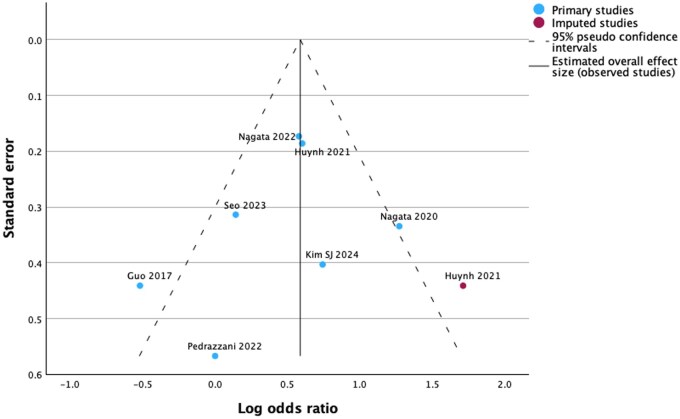
Results: Nine studies met inclusion criteria. All were retrospective cohort studies; most considered "conversion to open" as laparoscopic procedures. Pooled odds ratio was 1.61 (P = .011, I2 = 0.62), and HR was 1.24 (P < .001, I2 = 0.10) for developing peritoneal metastases. Risk of bias was assessed as low or moderate for all studies. Quality of evidence was low.
Conclusions: Laparoscopic colectomy is associated with an increased risk of peritoneal recurrence compared with open colectomy for T4 colon cancer. Although selection bias in these nonrandomized studies should favor laparoscopic surgery, LC was associated with an increased risk of peritoneal recurrence. LC should be approached with caution for cT4 colon cancer. Strategies to mitigate the risk of peritoneal recurrence in T4 colon cancer, such as neoadjuvant chemotherapy or adjuvant intraperitoneal chemotherapy, should be further explored in prospective studies.
期刊介绍:
The Oncologist® is dedicated to translating the latest research developments into the best multidimensional care for cancer patients. Thus, The Oncologist is committed to helping physicians excel in this ever-expanding environment through the publication of timely reviews, original studies, and commentaries on important developments. We believe that the practice of oncology requires both an understanding of a range of disciplines encompassing basic science related to cancer, translational research, and clinical practice, but also the socioeconomic and psychosocial factors that determine access to care and quality of life and function following cancer treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


