Paul Aujoulat, Jean Yves Le Reste, Benoit Chiron, Lucas Beurton-Couraud, Marie Barais, Pierre Barraine, Morgane Guillou-Landreat, Delphine Le Goff
{"title":"Risk factors for decompensation among multimorbid patients: analysis of a French Cohort with a 24-month follow-up.","authors":"Paul Aujoulat, Jean Yves Le Reste, Benoit Chiron, Lucas Beurton-Couraud, Marie Barais, Pierre Barraine, Morgane Guillou-Landreat, Delphine Le Goff","doi":"10.1017/S1463423625100157","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>The European General Practitioners Research Network (EGPRN) designed and validated a comprehensive definition of multimorbidity using a systematic literature review and qualitative research throughout Europe. Identification of risk factors for decompensation would be an interesting challenge for family physicians (FPs) in the management of multimorbid patients. The aim was to assess which items from the EGPRN's definition of multimorbidity could identify outpatients at risk of decompensation at 24 months.</p><p><strong>Methods: </strong>A cohort study. About 120 multimorbid patients from Western Brittany, France, were included by general practitioners between 2014 and 2015. The status \"decompensation\" (hospitalization of at least 7 days or death) or \"nothing to report (NTR)\" was collected at 24 months of follow-up.</p><p><strong>Findings: </strong>At 24 months, there were 44 patients (36.6%) in the decompensation group. Two variables were significant risk factors for decompensation: the number of visits to the FP per year (HR = 1.06 [95% CI 1.03-1.10], <i>P</i> < 0.001) and the total number of diseases (HR = 1.12 [95% CI 1.013-1.33], <i>P</i> = 0.039).</p><p><strong>Conclusion: </strong>FPs should be warned that a high number of consultations and a high total number of diseases may predict death or hospitalization. These results need to be confirmed by large-scale cohorts in primary care.</p>","PeriodicalId":74493,"journal":{"name":"Primary health care research & development","volume":"26 ","pages":"e60"},"PeriodicalIF":1.7000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281042/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Primary health care research & development","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/S1463423625100157","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
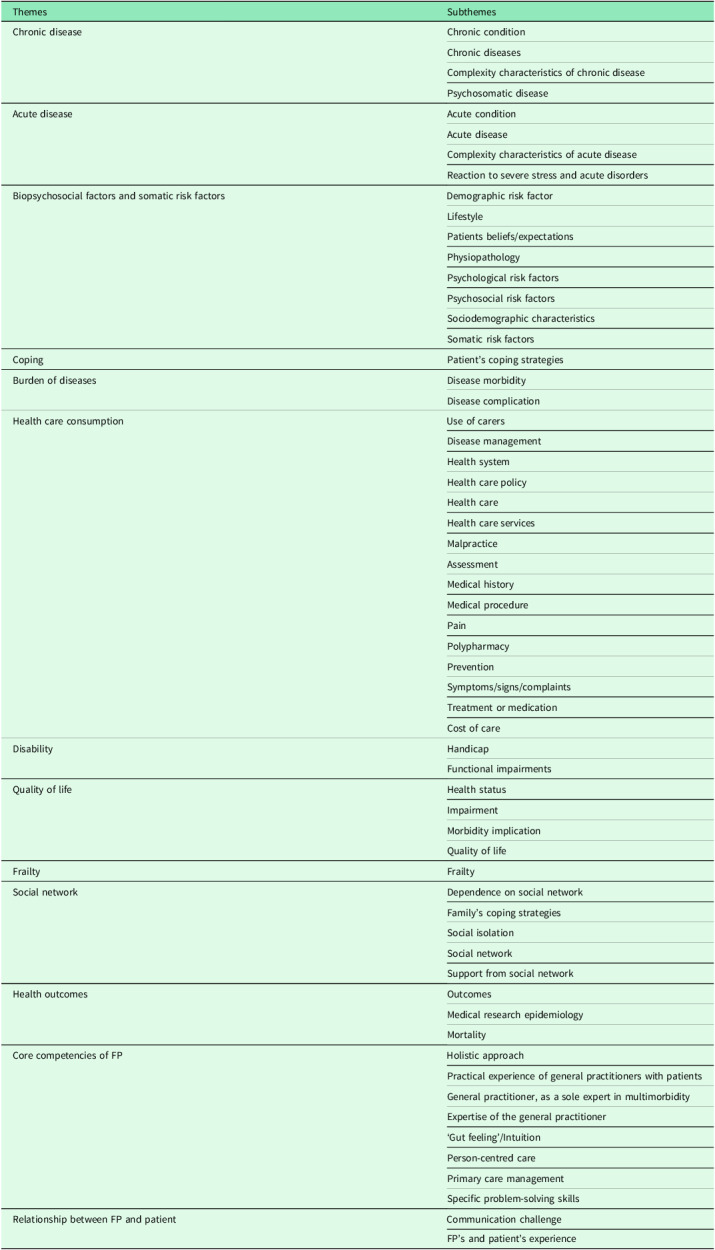
Aim: The European General Practitioners Research Network (EGPRN) designed and validated a comprehensive definition of multimorbidity using a systematic literature review and qualitative research throughout Europe. Identification of risk factors for decompensation would be an interesting challenge for family physicians (FPs) in the management of multimorbid patients. The aim was to assess which items from the EGPRN's definition of multimorbidity could identify outpatients at risk of decompensation at 24 months.
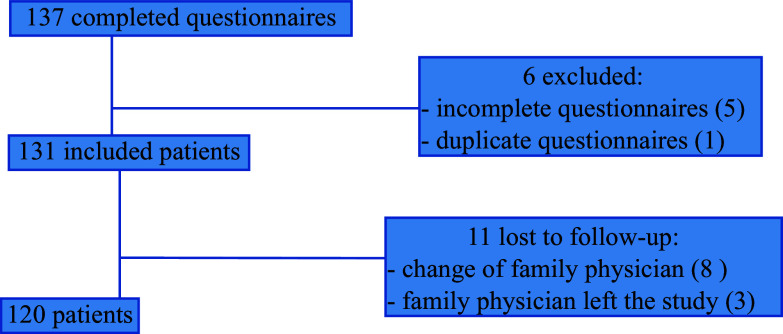
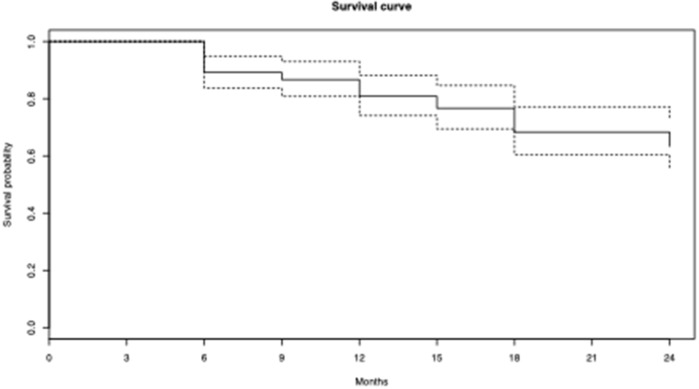
Methods: A cohort study. About 120 multimorbid patients from Western Brittany, France, were included by general practitioners between 2014 and 2015. The status "decompensation" (hospitalization of at least 7 days or death) or "nothing to report (NTR)" was collected at 24 months of follow-up.
Findings: At 24 months, there were 44 patients (36.6%) in the decompensation group. Two variables were significant risk factors for decompensation: the number of visits to the FP per year (HR = 1.06 [95% CI 1.03-1.10], P < 0.001) and the total number of diseases (HR = 1.12 [95% CI 1.013-1.33], P = 0.039).
Conclusion: FPs should be warned that a high number of consultations and a high total number of diseases may predict death or hospitalization. These results need to be confirmed by large-scale cohorts in primary care.
目的:欧洲全科医生研究网络(EGPRN)通过系统的文献回顾和全欧洲的定性研究,设计并验证了多病的综合定义。识别失代偿的危险因素将是家庭医生(FPs)管理多病患者的一个有趣的挑战。目的是评估EGPRN多病定义中的哪些项目可以识别24个月时有失代偿风险的门诊患者。方法:队列研究。2014年至2015年间,来自法国西布列塔尼的约120名多病患者被全科医生纳入研究。随访24个月时收集“失偿”(住院至少7天或死亡)或“无报告”状态。结果:24个月时,失代偿组44例(36.6%)。两个变量是失代偿的重要危险因素:每年到计划生育中心就诊的次数(HR = 1.06 [95% CI 1.03-1.10], P < 0.001)和疾病总数(HR = 1.12 [95% CI 1.013-1.33], P = 0.039)。结论:急诊患者应注意,高就诊次数和高疾病总数可能预示死亡或住院。这些结果需要在初级保健的大规模队列中得到证实。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


