{"title":"Measurement Bias in Documentation of Social Risk Among Medicare Beneficiaries.","authors":"Paula Chatterjee, Eliza Macneal, Eric T Roberts","doi":"10.1001/jamahealthforum.2025.1923","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Health care organizations are increasingly measuring social risk using Z codes. Types of social risk captured in Z codes include issues related to employment, housing, education, or other psychosocial circumstances. Prior work has found low use of Z codes overall, but measurement may be biased in other ways that have implications for risk adjustment and resource allocation.</p><p><strong>Objective: </strong>To characterize Z code measurement among hospitalized Medicare beneficiaries across levels of clinical complexity and historical health care utilization and examine implications of these patterns for mortality prediction.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study included Medicare beneficiaries with an inpatient hospital admission in 2022. Data were analyzed from May 2024 to June 2025.</p><p><strong>Main outcomes and measurements: </strong>Presence of Z codes (codes Z55 to Z65) in any diagnosis field for a hospital admission, variation in Z code documentation across beneficiaries categorized by clinical risk (Elixhauser Comorbidity Index risk scores and predicted 30-day mortality risk) and historical utilization levels (number of hospitalizations in the prior year), and the association between Z code documentation and observed 30-day mortality, controlling for hospital fixed effects.</p><p><strong>Results: </strong>Among 7 069 611 hospitalized Medicare beneficiaries in 2022, 3 816 420 (54.0%) were female, and 6 093 932 (86.1%) were 65 years or older. A total of 148 592 (2.1%) had at least 1 Z code on the index hospital claim. Within-hospital Z code prevalence was higher for beneficiaries with lower Elixhauser Comorbidity Index clinical risk scores (2.8% vs 1.5%) and higher among patients with at least 2 hospitalizations in the prior year (2.6%) than patients with zero (1.8%) or 1 (2.1%) prior hospitalizations. Despite known population-level associations between social risk and increased mortality, Z code prevalence was highest among beneficiaries with the lowest predicted 30-day mortality risk (4.4%) and lowest among beneficiaries with the highest mortality risk (1.6%). Correspondingly, in within-hospital analyses that did not adjust for patient-level covariates such as demographic characteristics and clinical risk, the presence of a Z code was associated with a lower probability of observed 30-day mortality (5.1% vs 4.2%; difference, -0.9 percentage points; 95% CI, -1.0 to -0.8).</p><p><strong>Conclusions and relevance: </strong>This cohort study found that Z code use patterns likely underrepresent social risk among clinically complex patients, resulting in a spurious negative association between documented social risk and mortality. Alternative socioeconomic indicators, including data collected for population and public health surveillance, may offer more reliable measures of social risk than Z codes.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 7","pages":"e251923"},"PeriodicalIF":11.3000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12274977/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.1923","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Health care organizations are increasingly measuring social risk using Z codes. Types of social risk captured in Z codes include issues related to employment, housing, education, or other psychosocial circumstances. Prior work has found low use of Z codes overall, but measurement may be biased in other ways that have implications for risk adjustment and resource allocation.
Objective: To characterize Z code measurement among hospitalized Medicare beneficiaries across levels of clinical complexity and historical health care utilization and examine implications of these patterns for mortality prediction.
Design, setting, and participants: This retrospective cohort study included Medicare beneficiaries with an inpatient hospital admission in 2022. Data were analyzed from May 2024 to June 2025.
Main outcomes and measurements: Presence of Z codes (codes Z55 to Z65) in any diagnosis field for a hospital admission, variation in Z code documentation across beneficiaries categorized by clinical risk (Elixhauser Comorbidity Index risk scores and predicted 30-day mortality risk) and historical utilization levels (number of hospitalizations in the prior year), and the association between Z code documentation and observed 30-day mortality, controlling for hospital fixed effects.
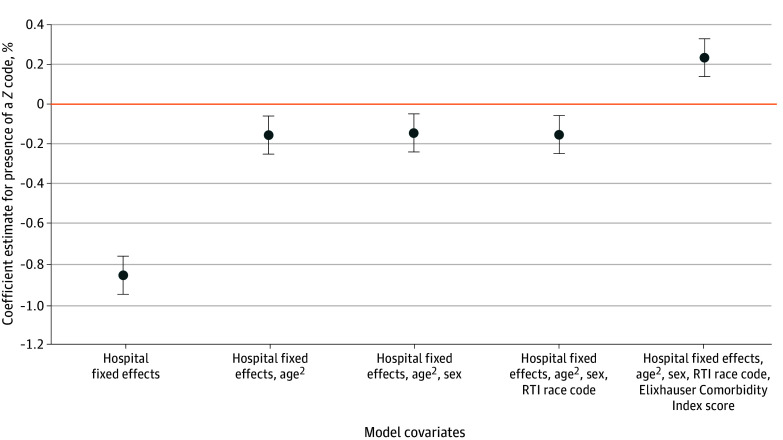
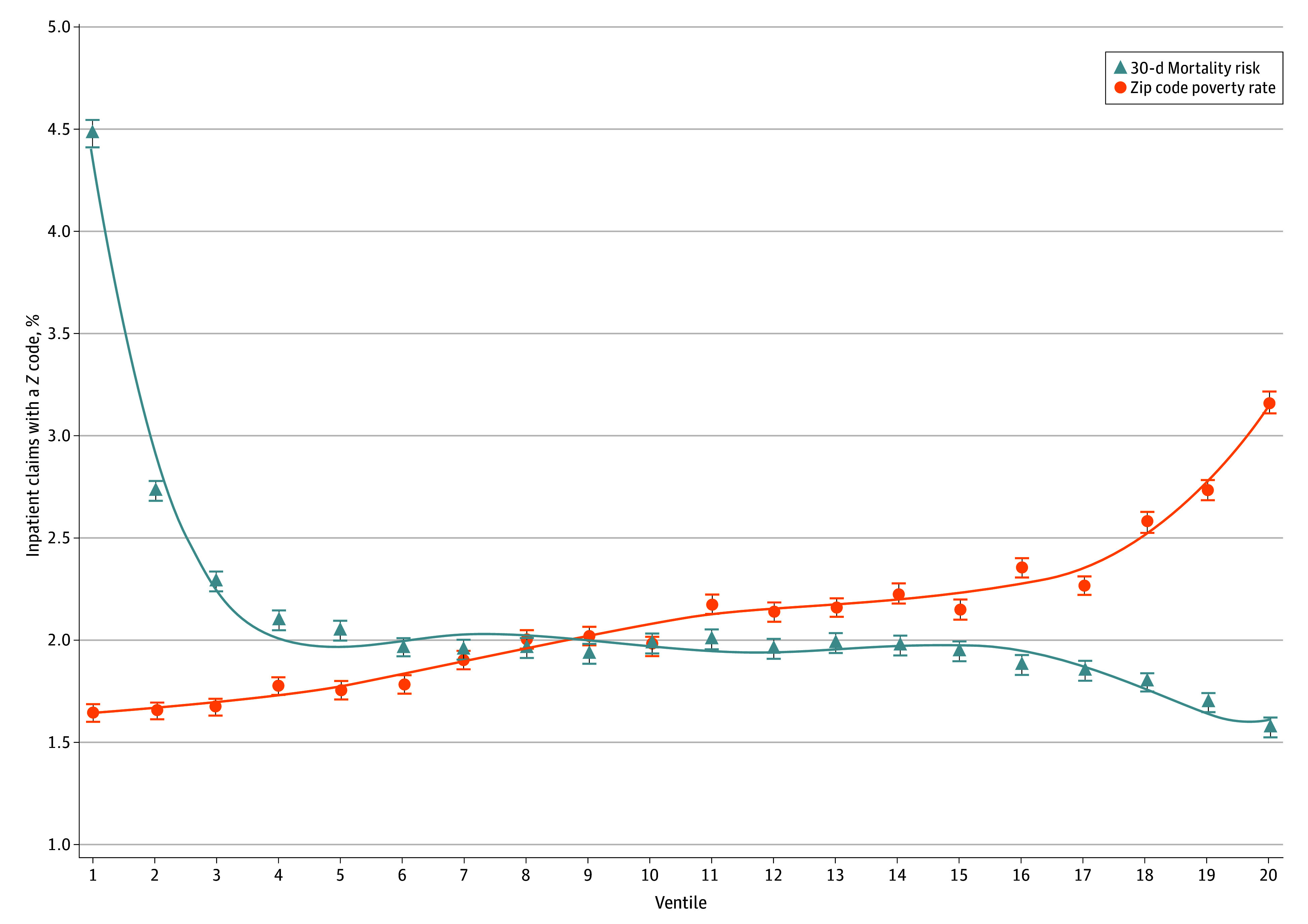
Results: Among 7 069 611 hospitalized Medicare beneficiaries in 2022, 3 816 420 (54.0%) were female, and 6 093 932 (86.1%) were 65 years or older. A total of 148 592 (2.1%) had at least 1 Z code on the index hospital claim. Within-hospital Z code prevalence was higher for beneficiaries with lower Elixhauser Comorbidity Index clinical risk scores (2.8% vs 1.5%) and higher among patients with at least 2 hospitalizations in the prior year (2.6%) than patients with zero (1.8%) or 1 (2.1%) prior hospitalizations. Despite known population-level associations between social risk and increased mortality, Z code prevalence was highest among beneficiaries with the lowest predicted 30-day mortality risk (4.4%) and lowest among beneficiaries with the highest mortality risk (1.6%). Correspondingly, in within-hospital analyses that did not adjust for patient-level covariates such as demographic characteristics and clinical risk, the presence of a Z code was associated with a lower probability of observed 30-day mortality (5.1% vs 4.2%; difference, -0.9 percentage points; 95% CI, -1.0 to -0.8).
Conclusions and relevance: This cohort study found that Z code use patterns likely underrepresent social risk among clinically complex patients, resulting in a spurious negative association between documented social risk and mortality. Alternative socioeconomic indicators, including data collected for population and public health surveillance, may offer more reliable measures of social risk than Z codes.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


