Comparative Cost Analysis for Direct Medical Costs of Protocol Administration of Non-Small Cell Lung Cancer Treatment Regimens in Curative Intent: A Micro-Costing Study in Jordan.
Saba S Madae'en, Ahmed A Salem, Naila S Ararawi, Ezaldeen J Ramzi, Roa'a F Aloueedat, Abdullah M Saabenh, Diala A Allouzi, Reem H Abuoudeh, Osama E Hnaif, Leen M Musa, Salma H Alshdaifat, Ahmad J Al-Tanashat, Hala Y Almasa'afeh, Salma M Abuallaban
{"title":"Comparative Cost Analysis for Direct Medical Costs of Protocol Administration of Non-Small Cell Lung Cancer Treatment Regimens in Curative Intent: A Micro-Costing Study in Jordan.","authors":"Saba S Madae'en, Ahmed A Salem, Naila S Ararawi, Ezaldeen J Ramzi, Roa'a F Aloueedat, Abdullah M Saabenh, Diala A Allouzi, Reem H Abuoudeh, Osama E Hnaif, Leen M Musa, Salma H Alshdaifat, Ahmad J Al-Tanashat, Hala Y Almasa'afeh, Salma M Abuallaban","doi":"10.2147/CEOR.S520119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-small cell lung cancer (NSCLC) treatment costs significantly impact healthcare systems. This study analyzes direct costs and cost drivers of perioperative and adjuvant systemic treatments for stage I-II NSCLC from Jordanian healthcare providers' perspective using micro-costing methodology.</p><p><strong>Methods: </strong>We employed micro-costing to analyze direct medical expenses including drug acquisition, preparation, administration, pre/post-medications, diagnostics, labor, and wastage costs for perioperative regimens used in stage I-II NSCLC. International guidelines defined therapeutic regimens, while drug prices were extracted from Jordan Food and Drug Administration's database. Published data and surveys quantified micro-costs.</p><p><strong>Results: </strong>Among 26 assessed regimens (2 targeted therapy, 10 chemotherapy, 10 chemo-immunotherapy, 4 immunotherapy), targeted/immunotherapy agents significantly increased costs. Chemotherapy regimen cost differences ranged from $633.68 (squamous) to $1,763.91 (non-squamous) per cycle. Antineoplastic agents were primary cost drivers, highest for Durvalumab (98.72% of cycle cost). Laboratory costs comprised up to 50.73% in chemotherapy and 7.24% in immunotherapy regimens. Wastage contributed up to 10.36% of total cycle costs. Average administration cost was $35 per cycle. Maximum cycle costs were: targeted therapy (Osimertinib) $7,206.44, immunotherapy (Durvalumab) $9,057.71, immune-chemotherapy (Durvalumab-Carboplatin-Pemetrexed) $11,358.43, and chemotherapy (Carboplatin-Pemetrexed) $2,300.72.</p><p><strong>Conclusion: </strong>Our results highlight the substantial economic impact and cost variability among treatment regimens. This variability presents opportunities for cost reduction through careful selection of therapeutically equivalent regimens based on pricing and toxicity profiles. The findings emphasize the need for comprehensive and precise cost analysis to inform healthcare policies and clinical practices. Future research should focus on cost-effectiveness analyses of these expensive agents to ensure value for money, support evidence-based decision-making, and strengthen price negotiations with suppliers.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"455-471"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267825/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S520119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Non-small cell lung cancer (NSCLC) treatment costs significantly impact healthcare systems. This study analyzes direct costs and cost drivers of perioperative and adjuvant systemic treatments for stage I-II NSCLC from Jordanian healthcare providers' perspective using micro-costing methodology.
Methods: We employed micro-costing to analyze direct medical expenses including drug acquisition, preparation, administration, pre/post-medications, diagnostics, labor, and wastage costs for perioperative regimens used in stage I-II NSCLC. International guidelines defined therapeutic regimens, while drug prices were extracted from Jordan Food and Drug Administration's database. Published data and surveys quantified micro-costs.
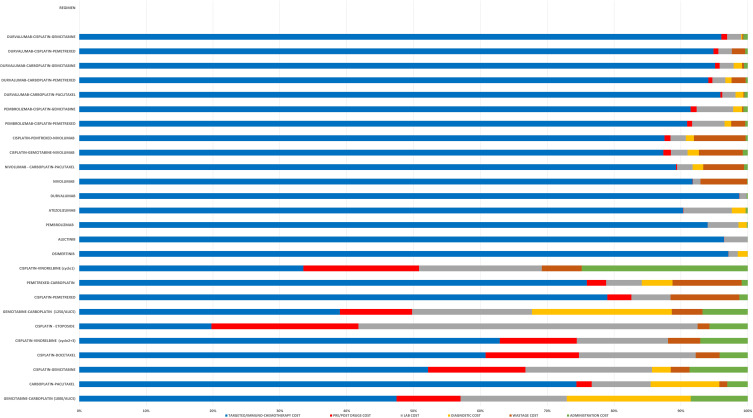
Results: Among 26 assessed regimens (2 targeted therapy, 10 chemotherapy, 10 chemo-immunotherapy, 4 immunotherapy), targeted/immunotherapy agents significantly increased costs. Chemotherapy regimen cost differences ranged from $633.68 (squamous) to $1,763.91 (non-squamous) per cycle. Antineoplastic agents were primary cost drivers, highest for Durvalumab (98.72% of cycle cost). Laboratory costs comprised up to 50.73% in chemotherapy and 7.24% in immunotherapy regimens. Wastage contributed up to 10.36% of total cycle costs. Average administration cost was $35 per cycle. Maximum cycle costs were: targeted therapy (Osimertinib) $7,206.44, immunotherapy (Durvalumab) $9,057.71, immune-chemotherapy (Durvalumab-Carboplatin-Pemetrexed) $11,358.43, and chemotherapy (Carboplatin-Pemetrexed) $2,300.72.
Conclusion: Our results highlight the substantial economic impact and cost variability among treatment regimens. This variability presents opportunities for cost reduction through careful selection of therapeutically equivalent regimens based on pricing and toxicity profiles. The findings emphasize the need for comprehensive and precise cost analysis to inform healthcare policies and clinical practices. Future research should focus on cost-effectiveness analyses of these expensive agents to ensure value for money, support evidence-based decision-making, and strengthen price negotiations with suppliers.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


