Advancing Health Equity for American Indian and Alaska Native People Through Inclusion in Clinical Trials: Anti-SARS-CoV-2 Monoclonal Antibody Treatment and COVID-19 Outcomes Among Ambulatory Cherokee Nation Health Services Patients.
IF 2.5 Q2 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Jorge Mera, Whitney Essex, Elizabeth Menstell Coyle, Ashley Comiford, Molly A Feder
{"title":"Advancing Health Equity for American Indian and Alaska Native People Through Inclusion in Clinical Trials: Anti-SARS-CoV-2 Monoclonal Antibody Treatment and COVID-19 Outcomes Among Ambulatory Cherokee Nation Health Services Patients.","authors":"Jorge Mera, Whitney Essex, Elizabeth Menstell Coyle, Ashley Comiford, Molly A Feder","doi":"10.1089/heq.2024.0185","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Racial/ethnic minority groups are underrepresented in clinical trials with American Indian and Alaska Native (AI/AN) people having the lowest representation. This article aims to contribute to the literature to address that gap by sharing the results of the use of anti-SARS-CoV-2 monoclonal antibodies among AI/AN people at risk for severe COVID-19.</p><p><strong>Methods: </strong>This retrospective cohort study assessed data from ambulatory AI/AN patients enrolled in Cherokee Nation Health Services in Northeastern Oklahoma, who had a positive test for SARS-CoV-2, high risk for progression, and were offered anti-SARS-CoV-2 monoclonal antibody treatment active against the circulating SARS-CoV-2 strain from December 1, 2020, to April 16, 2021. The outcomes of interest were all-cause and COVID-19-related emergency department visits, hospitalizations, intensive care admissions, and deaths within 28 days of being offered treatment.</p><p><strong>Results: </strong>Among 1,447 participants, 813 (56.2%) were treated and 634 (43.8%) were not. When adjusted for potential confounders, there was a significant difference in the odds of treated versus untreated patients experiencing a COVID-19-related emergency department visit (OR, 0.42; 95% CI, 0.27-0.63) and hospitalization (OR, 0.10; 95% CI, 0.03-0.31).</p><p><strong>Discussion: </strong>Anti-SARS-CoV-2 monoclonal antibody treatment was associated with lower odds of COVID-19-related emergency department visits and hospitalization among high-risk AI/AN patients.</p><p><strong>Health equity implications: </strong>To advance health equity, it is critical to have representation of AI/AN in clinical trials and other research. This project is an example of how community partnerships with AI/AN health systems can strengthen the evidence for new and emerging treatments, address past harm, and advance equity.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"9 1","pages":"235-244"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12270532/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/heq.2024.0185","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Racial/ethnic minority groups are underrepresented in clinical trials with American Indian and Alaska Native (AI/AN) people having the lowest representation. This article aims to contribute to the literature to address that gap by sharing the results of the use of anti-SARS-CoV-2 monoclonal antibodies among AI/AN people at risk for severe COVID-19.
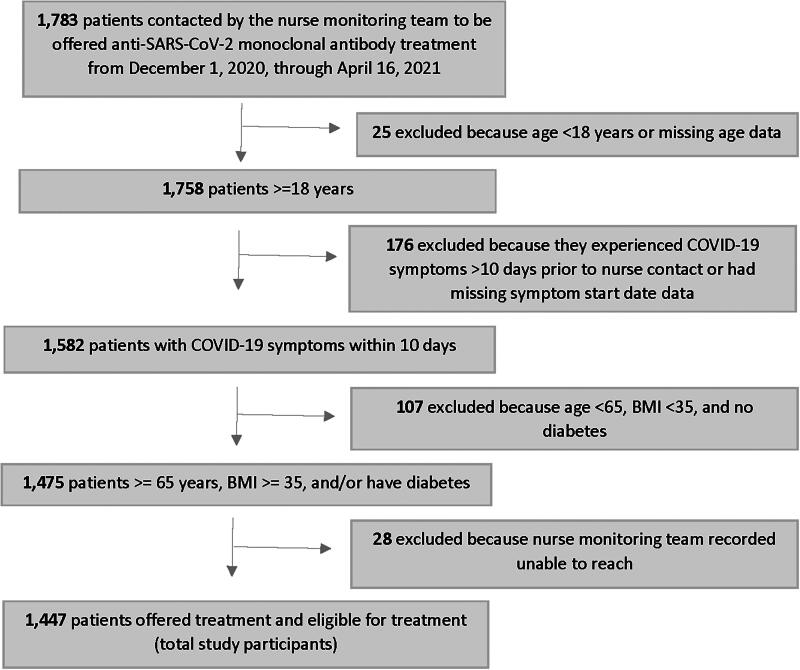
Methods: This retrospective cohort study assessed data from ambulatory AI/AN patients enrolled in Cherokee Nation Health Services in Northeastern Oklahoma, who had a positive test for SARS-CoV-2, high risk for progression, and were offered anti-SARS-CoV-2 monoclonal antibody treatment active against the circulating SARS-CoV-2 strain from December 1, 2020, to April 16, 2021. The outcomes of interest were all-cause and COVID-19-related emergency department visits, hospitalizations, intensive care admissions, and deaths within 28 days of being offered treatment.
Results: Among 1,447 participants, 813 (56.2%) were treated and 634 (43.8%) were not. When adjusted for potential confounders, there was a significant difference in the odds of treated versus untreated patients experiencing a COVID-19-related emergency department visit (OR, 0.42; 95% CI, 0.27-0.63) and hospitalization (OR, 0.10; 95% CI, 0.03-0.31).
Discussion: Anti-SARS-CoV-2 monoclonal antibody treatment was associated with lower odds of COVID-19-related emergency department visits and hospitalization among high-risk AI/AN patients.
Health equity implications: To advance health equity, it is critical to have representation of AI/AN in clinical trials and other research. This project is an example of how community partnerships with AI/AN health systems can strengthen the evidence for new and emerging treatments, address past harm, and advance equity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


