Electroencephalographic changes related to cortico-subcortical decoupling during propofol-induced loss of consciousness: A secondary analysis of a prospective observational study
IF 5.1
2区 医学
Q1 ANESTHESIOLOGY
引用次数: 0
Abstract
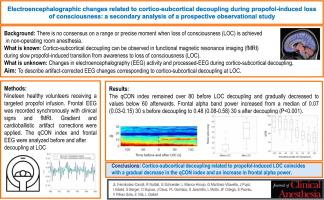
Background
Cortico-subcortical decoupling has been observed in functional magnetic resonance imaging (fMRI) during slow propofol-induced loss of consciousness (LOC). However, corresponding electroencephalography (EEG) free of the cardioballistic and fMRI artifacts is essential for translating decoupling observations to clinical monitoring.
Objective
To describe artifact-corrected EEG changes corresponding to cortico-subcortical decoupling at LOC.
Design
Secondary analysis of a prospective observational study.
Setting
Tertiary-care hospital, data collection from June 2017 to January 2019.
Participants
Nineteen healthy volunteers receiving a targeted propofol infusion.
Interventions
Frontal EEG was recorded synchronously with clinical signs and fMRI. Gradient artifact correction was based on iterative peak detection. Cardioballistic artifact correction was accomplished with a recently described algorithmic method based on peak detection combined with temporal constraints.
Main outcome measures
The qCON index and frontal EEG before and after decoupling at LOC.
Results
Algorithm-filtered EEG tracings were suitable for analysis in 16 subjects. Propofol-induced LOC was achieved at a median (IQR) target plasma concentration of 4.5 (3.91 to 4.61) μg/mL and an effect-site concentration of 4.0 (2.94 to 4.31) μg/mL. The qCON index remained over 80 before decoupling and gradually decreased to values below 60 afterwards. Frontal alpha band power increased significantly from a median of 0.07 (0.03 to 0.15) 30 s before decoupling to 0.48 (0.08 to 0.58) 30 s after decoupling (p < 0.001).
Conclusions
Cortico-subcortical decoupling related to propofol-induced LOC coincides with a gradual decrease in the qCON index and an increase in frontal alpha power. These results help translate fMRI findings to bedside settings.
Registered at EudraCT (reference 2016–004833-25). Principal Investigator: Juan L. Fernández-Candil. Date of registration: January 4, 2017. Start Date: June 13, 2017.
异丙酚诱导的意识丧失期间与皮质-皮质下解耦相关的脑电图变化:一项前瞻性观察研究的二次分析
在异丙酚诱导的缓慢意识丧失(LOC)过程中,功能磁共振成像(fMRI)观察到皮质-皮质下解耦。然而,相应的脑电图(EEG)无心电和功能磁共振伪影是将解耦观察转化为临床监测所必需的。目的描述脑皮层与皮层下解耦后的伪影校正脑电图变化。设计前瞻性观察性研究的二次分析。三级医院,数据收集时间为2017年6月至2019年1月。参与者:19名健康志愿者接受定向异丙酚输注。干预措施:额叶脑电图与临床体征、功能磁共振成像同步记录。基于迭代峰检测的梯度伪影校正。最近提出了一种基于峰值检测和时间约束相结合的算法来完成心脏学伪影校正。主要观察指标LOC解耦前后的qCON指数和额叶脑电图。结果算法滤波后的脑电描记适于分析16例受试者。异丙酚诱导LOC的中位(IQR)靶血浆浓度为4.5 (3.91 ~ 4.61)μg/mL,效应位点浓度为4.0 (2.94 ~ 4.31)μg/mL。脱钩前qCON指数保持在80以上,脱钩后逐渐下降至60以下。正面alpha波段功率中位数从去耦前的0.07 (0.03 ~ 0.15)30s显著增加到去耦后的0.48 (0.08 ~ 0.58)30s (p <;0.001)。结论异丙酚诱导LOC的皮质-皮质下解耦与qCON指数的逐渐降低和额叶α功率的增加相一致。这些结果有助于将fMRI结果转化为床边设置。注册于EudraCT(参考文献2016-004833-25)。首席研究员:Juan L. Fernández-Candil。报名日期:2017年1月4日。开始日期:2017年6月13日。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

CiteScore
7.40
自引率
4.50%
发文量
346
审稿时长
23 days
期刊介绍:
The Journal of Clinical Anesthesia (JCA) addresses all aspects of anesthesia practice, including anesthetic administration, pharmacokinetics, preoperative and postoperative considerations, coexisting disease and other complicating factors, cost issues, and similar concerns anesthesiologists contend with daily. Exceptionally high standards of presentation and accuracy are maintained.
The core of the journal is original contributions on subjects relevant to clinical practice, and rigorously peer-reviewed. Highly respected international experts have joined together to form the Editorial Board, sharing their years of experience and clinical expertise. Specialized section editors cover the various subspecialties within the field. To keep your practical clinical skills current, the journal bridges the gap between the laboratory and the clinical practice of anesthesiology and critical care to clarify how new insights can improve daily practice.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


