Luise Tittl, Christina Köhler, Sandra Marten, Christiane Naue, Jan Beyer-Westendorf
{"title":"Venous Thromboembolism Therapy with Edoxaban in Daily Care Patients: Results from the DRESDEN NOAC REGISTRY.","authors":"Luise Tittl, Christina Köhler, Sandra Marten, Christiane Naue, Jan Beyer-Westendorf","doi":"10.1055/a-2635-4840","DOIUrl":null,"url":null,"abstract":"<p><p>Direct oral anticoagulants such as edoxaban are standard of care in current treatment of venous thromboembolism (VTE). However, phase III trial data need confirmation in real-world settings. We extracted data from the prospective, noninterventional multiple-indication DRESDEN NOAC REGISTRY to evaluate outcome rates during VTE treatment with edoxaban. Patients were included in this analysis, if they had acute VTE and if patient enrolment and edoxaban initiation occurred within 30 days after VTE diagnosis. Patient characteristics, treatment persistence, and clinical outcomes were centrally adjudicated using standard definitions. Until December 31, 2023, 323 acute VTE patients (median age 67 years, 56.7% male) were enrolled and initiated edoxaban within 7.8 ± 4.9 days (mean) for isolated deep vein thrombosis (DVT) (57.6%) or pulmonary embolism (PE) ± DVT (42.4%). Mean duration of follow-up was 3.9 ± 1.9 years with a mean duration of edoxaban exposure of 1.5 ± 1.7 years. During ongoing edoxaban therapy, 3/323 patients (0.9%) experienced recurrent VTE (0.6/100 patient-years); 141/323 (43.7%) patients reported clinically relevant International Society on Thrombosis and Haemostasis (ISTH) nonmajor bleeding and 16 reported ISTH major bleeding (5.0%; 3.2/100 patient-years). Death was observed in 53 patients (4.1/100 patient-years). At 6 months, 78.2% were still taking edoxaban, 2% were electively switched to dose-reduced secondary prophylaxis with apixaban 2.5 mg twice a day or rivaroxaban 10 mg once daily. The remaining patients had a scheduled end of VTE treatment (11.4%) or were switched to nonedoxaban therapeutic anticoagulation (6.2%). Our results indicate effectiveness of edoxaban in acute VTE treatment with excellent persistence in the treatment and low rates of unplanned discontinuation. Bleeding was frequently observed, but rates of major bleeding were low and comparable to phase III data.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"9 ","pages":"a26354840"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12265392/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2635-4840","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
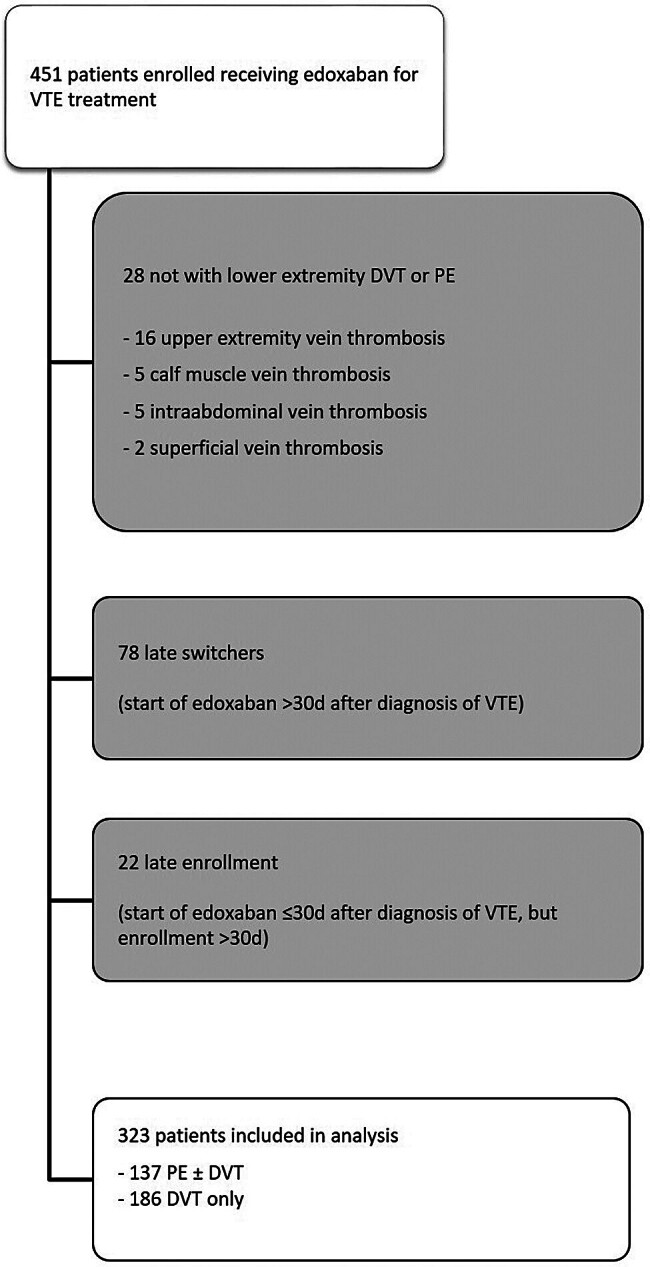
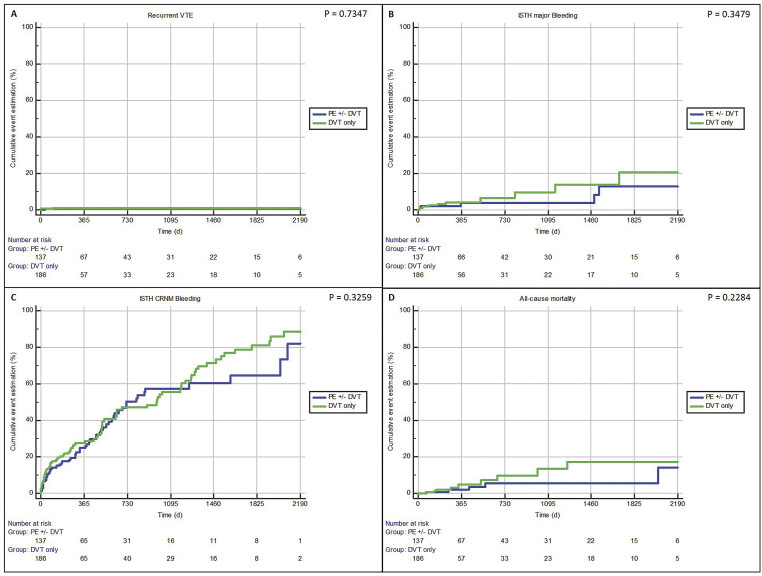
Direct oral anticoagulants such as edoxaban are standard of care in current treatment of venous thromboembolism (VTE). However, phase III trial data need confirmation in real-world settings. We extracted data from the prospective, noninterventional multiple-indication DRESDEN NOAC REGISTRY to evaluate outcome rates during VTE treatment with edoxaban. Patients were included in this analysis, if they had acute VTE and if patient enrolment and edoxaban initiation occurred within 30 days after VTE diagnosis. Patient characteristics, treatment persistence, and clinical outcomes were centrally adjudicated using standard definitions. Until December 31, 2023, 323 acute VTE patients (median age 67 years, 56.7% male) were enrolled and initiated edoxaban within 7.8 ± 4.9 days (mean) for isolated deep vein thrombosis (DVT) (57.6%) or pulmonary embolism (PE) ± DVT (42.4%). Mean duration of follow-up was 3.9 ± 1.9 years with a mean duration of edoxaban exposure of 1.5 ± 1.7 years. During ongoing edoxaban therapy, 3/323 patients (0.9%) experienced recurrent VTE (0.6/100 patient-years); 141/323 (43.7%) patients reported clinically relevant International Society on Thrombosis and Haemostasis (ISTH) nonmajor bleeding and 16 reported ISTH major bleeding (5.0%; 3.2/100 patient-years). Death was observed in 53 patients (4.1/100 patient-years). At 6 months, 78.2% were still taking edoxaban, 2% were electively switched to dose-reduced secondary prophylaxis with apixaban 2.5 mg twice a day or rivaroxaban 10 mg once daily. The remaining patients had a scheduled end of VTE treatment (11.4%) or were switched to nonedoxaban therapeutic anticoagulation (6.2%). Our results indicate effectiveness of edoxaban in acute VTE treatment with excellent persistence in the treatment and low rates of unplanned discontinuation. Bleeding was frequently observed, but rates of major bleeding were low and comparable to phase III data.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


