Christina-Le Nguyen, Wai Chung Tse, Thomas M Carney, Alayna Carrandi, Mussab Fagery, Alisa M Higgins
{"title":"Health Economic Evaluations in Intensive Care: An Updated Systematic Review.","authors":"Christina-Le Nguyen, Wai Chung Tse, Thomas M Carney, Alayna Carrandi, Mussab Fagery, Alisa M Higgins","doi":"10.1097/CCE.0000000000001288","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Intensive care is a critical but resource-intensive component of healthcare. Health economic evaluations, such as cost-effectiveness analyses (CEAs), offer valuable insights for decision-making by weighing the costs and benefits of various healthcare interventions. We aimed to identify and summarize the existing health economic evaluations within intensive care and identify areas for future research.</p><p><strong>Data sources: </strong>We searched six academic databases to identify full health economic evaluations of ICU interventions published between 1993 and 2023. Databases included: Ovid (MEDLINE, Embase, and evidence based medicine (EBM) Reviews [Health Technology Assessments and National Health Service (NHS) Economic Evaluation Database]), EBSCO (CINAHL and EconLit), and Web of Science.</p><p><strong>Study selection: </strong>Health economic evaluations of interventions for adult patients in the ICU were included. Economic evaluations include CEAs, cost-utility, cost-benefit, and cost-minimization analyses, while pediatric, animal and weaning center studies were excluded.</p><p><strong>Data extraction: </strong>Data were extracted by two independent reviewers. Study quality was assessed using the Consolidated Health Economic Evaluation Reporting Standards checklist.</p><p><strong>Data synthesis: </strong>We identified 219 relevant studies published between 1993 and 2023, with a significant rise in publications over the last decade. Most studies (97%) had good to excellent reporting quality. Incremental cost-effectiveness ratios (ICERs) ranged from dominant (more effective and less expensive) to $753,874 per life saved. ICERs for both cost per quality-adjusted life-years and cost per life-year gained ranged from dominant to dominated (more costly and less effective). Three studies (1%) were published in low- and middle-income countries (LMICs) and 58% of studies were modeling studies.</p><p><strong>Conclusions: </strong>Despite the importance of economic evidence in healthcare decision-making, there is a relative scarcity of cost-effectiveness studies in intensive care compared with other medical fields. Available economic evaluations in intensive care are characterized by significant heterogeneity. The wide range of ICERs for life saved, life-years gained, and quality-adjusted life-years reflects the diversity of ICU patients, interventions, and evaluation methods. Future research in LMICs and increasing trial-based research is recommended.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 7","pages":"e1288"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12269819/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001288","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Intensive care is a critical but resource-intensive component of healthcare. Health economic evaluations, such as cost-effectiveness analyses (CEAs), offer valuable insights for decision-making by weighing the costs and benefits of various healthcare interventions. We aimed to identify and summarize the existing health economic evaluations within intensive care and identify areas for future research.
Data sources: We searched six academic databases to identify full health economic evaluations of ICU interventions published between 1993 and 2023. Databases included: Ovid (MEDLINE, Embase, and evidence based medicine (EBM) Reviews [Health Technology Assessments and National Health Service (NHS) Economic Evaluation Database]), EBSCO (CINAHL and EconLit), and Web of Science.
Study selection: Health economic evaluations of interventions for adult patients in the ICU were included. Economic evaluations include CEAs, cost-utility, cost-benefit, and cost-minimization analyses, while pediatric, animal and weaning center studies were excluded.
Data extraction: Data were extracted by two independent reviewers. Study quality was assessed using the Consolidated Health Economic Evaluation Reporting Standards checklist.
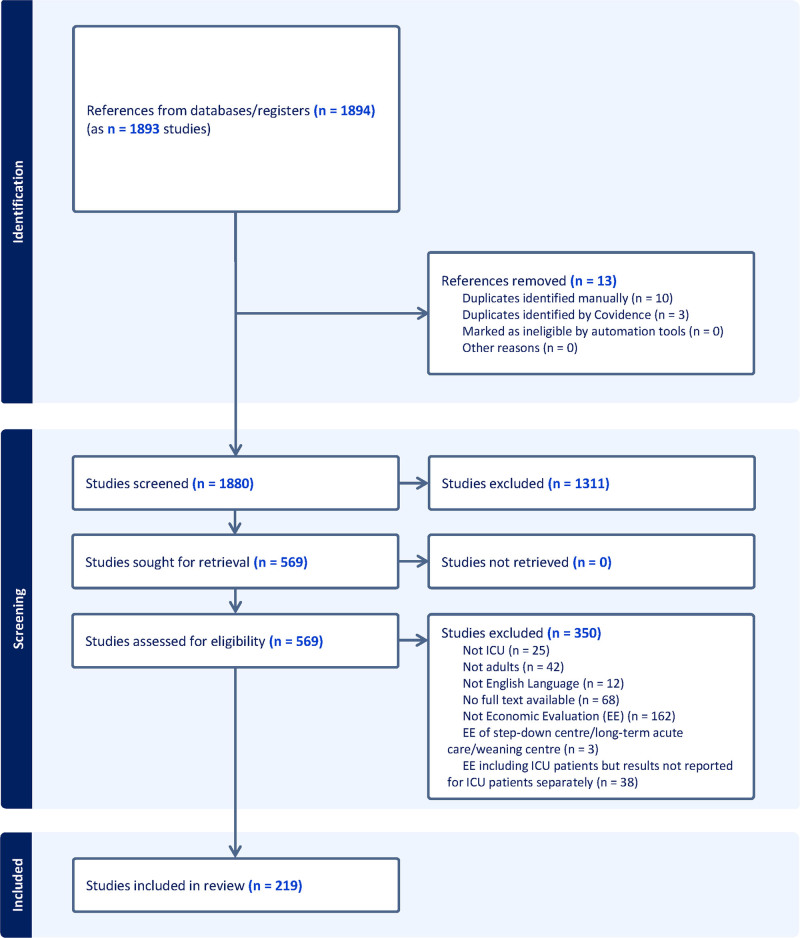
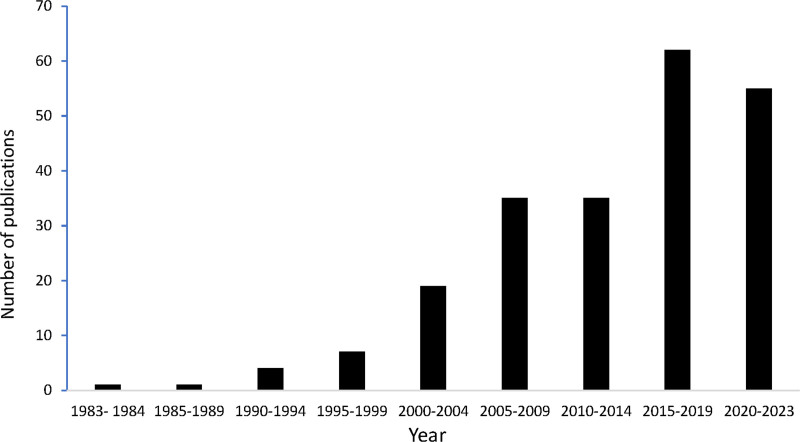
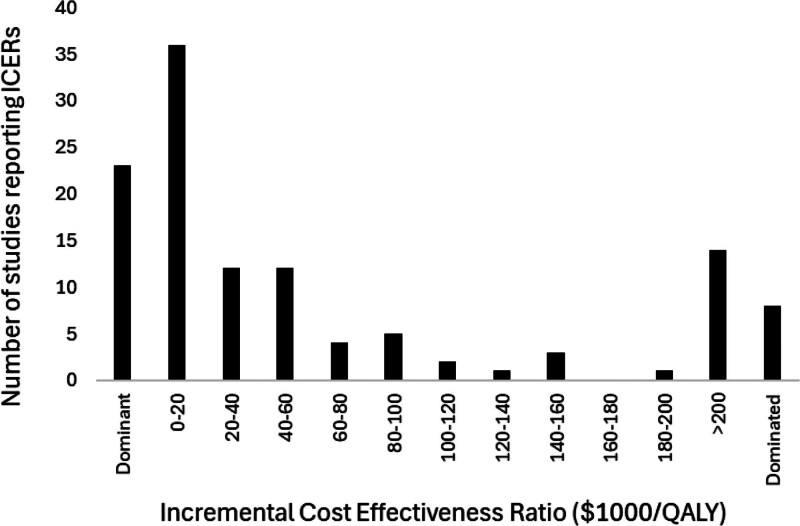
Data synthesis: We identified 219 relevant studies published between 1993 and 2023, with a significant rise in publications over the last decade. Most studies (97%) had good to excellent reporting quality. Incremental cost-effectiveness ratios (ICERs) ranged from dominant (more effective and less expensive) to $753,874 per life saved. ICERs for both cost per quality-adjusted life-years and cost per life-year gained ranged from dominant to dominated (more costly and less effective). Three studies (1%) were published in low- and middle-income countries (LMICs) and 58% of studies were modeling studies.
Conclusions: Despite the importance of economic evidence in healthcare decision-making, there is a relative scarcity of cost-effectiveness studies in intensive care compared with other medical fields. Available economic evaluations in intensive care are characterized by significant heterogeneity. The wide range of ICERs for life saved, life-years gained, and quality-adjusted life-years reflects the diversity of ICU patients, interventions, and evaluation methods. Future research in LMICs and increasing trial-based research is recommended.
目的:重症监护是医疗保健的关键但资源密集的组成部分。卫生经济评估,如成本效益分析(cea),通过权衡各种卫生保健干预措施的成本和收益,为决策提供了有价值的见解。我们的目的是识别和总结重症监护中现有的健康经济评估,并确定未来研究的领域。数据来源:我们检索了六个学术数据库,以确定1993年至2023年间发表的ICU干预措施的完整健康经济评估。数据库包括:Ovid (MEDLINE、Embase和循证医学(EBM)综述[卫生技术评估和国民健康服务(NHS)经济评估数据库])、EBSCO (CINAHL和EconLit)和Web of Science。研究选择:纳入对ICU成年患者干预措施的健康经济评价。经济评价包括cea、成本效用、成本效益和成本最小化分析,而排除了儿科、动物和断奶中心的研究。数据提取:数据由两名独立审稿人提取。采用综合卫生经济评价报告标准清单评估研究质量。数据综合:我们确定了1993年至2023年间发表的219项相关研究,在过去十年中出版物显著增加。大多数研究(97%)报告质量良好至优秀。增量成本效益比(ICERs)从占主导地位(更有效和更便宜)到每拯救一条生命的753,874美元不等。每质量调整生命年成本和每生命年获得成本的ICERs从占主导地位到占主导地位(成本更高,效果更差)。在低收入和中等收入国家发表了三项研究(1%),58%的研究是模型研究。结论:尽管经济证据在医疗保健决策中的重要性,但与其他医学领域相比,重症监护的成本效益研究相对缺乏。现有的重症监护经济评估具有显著的异质性。ICERs对挽救生命、获得生命年和质量调整生命年的广泛评估反映了ICU患者、干预措施和评估方法的多样性。建议今后在中低收入国家开展研究,并增加基于试验的研究。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


