{"title":"Phrenic nerve reconstruction after combined resection in malignant tumors: a narrative review.","authors":"Yosuke Hamada, Sakashi Fujimori, Souichiro Suzuki, Takahiro Karasaki, Shinichiro Kikunaga, Shusei Mihara","doi":"10.21037/med-25-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Phrenic nerve resection is sometimes necessary during tumor removal when the nerve is infiltrated by malignancies. However, this can result in diaphragmatic paralysis and respiratory insufficiency. While mechanical ventilation and diaphragmatic pacing may temporarily support respiratory function, phrenic nerve reconstruction offers a potential long-term solution. Nevertheless, its use during tumor resection remains underreported. This review assesses current evidence on phrenic nerve reconstruction, focusing on surgical techniques, nerve graft selection, and the feasibility of minimally invasive approaches.</p><p><strong>Methods: </strong>A literature search was conducted in PubMed for phrenic nerve reconstruction studies. English-language studies published between January 1, 1980 and January 30, 2025, that focused on immediate phrenic nerve reconstruction following tumor resection were included in the review.</p><p><strong>Key content and findings: </strong>Phrenic nerve reconstruction can be performed either immediately after nerve resection or as a delayed procedure. Immediate reconstruction, especially when conducted concurrently with tumor resection, has been shown to promote optimal nerve regeneration and functional recovery. In contrast, delayed reconstruction is generally associated with greater technical challenges and less predictable outcomes. Direct anastomosis is preferable when feasible; however, nerve grafting is often required due to insufficient residual nerve length to achieve a tension-free repair. Among graft options, the intercostal nerve is favorable due to its anatomical proximity and minimal additional surgical burden, whereas the use of other nerves, such as the sural nerve, requires an additional incision at a separate site, which may be less desirable. Successful reconstruction can also be achieved using minimally invasive approaches such as video-assisted thoracoscopic surgery (VATS) and robotic-assisted thoracoscopic surgery (RATS). Notably, the additional time required for reconstruction in minimally invasive procedures is manageable and does not significantly affect patient outcomes.</p><p><strong>Conclusions: </strong>Immediate phrenic nerve reconstruction, either by direct suturing or intercostal nerve grafting, is a feasible and effective method for preserving respiratory function. The ability to perform reconstruction using minimally invasive techniques further supports its clinical adoption. Given its advantages in functional recovery and its relatively low additional surgical burden, phrenic nerve resection followed by immediate reconstruction may be considered in most cases involving phrenic nerve invasion.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"9 ","pages":"15"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12260954/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-25-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Phrenic nerve resection is sometimes necessary during tumor removal when the nerve is infiltrated by malignancies. However, this can result in diaphragmatic paralysis and respiratory insufficiency. While mechanical ventilation and diaphragmatic pacing may temporarily support respiratory function, phrenic nerve reconstruction offers a potential long-term solution. Nevertheless, its use during tumor resection remains underreported. This review assesses current evidence on phrenic nerve reconstruction, focusing on surgical techniques, nerve graft selection, and the feasibility of minimally invasive approaches.
Methods: A literature search was conducted in PubMed for phrenic nerve reconstruction studies. English-language studies published between January 1, 1980 and January 30, 2025, that focused on immediate phrenic nerve reconstruction following tumor resection were included in the review.
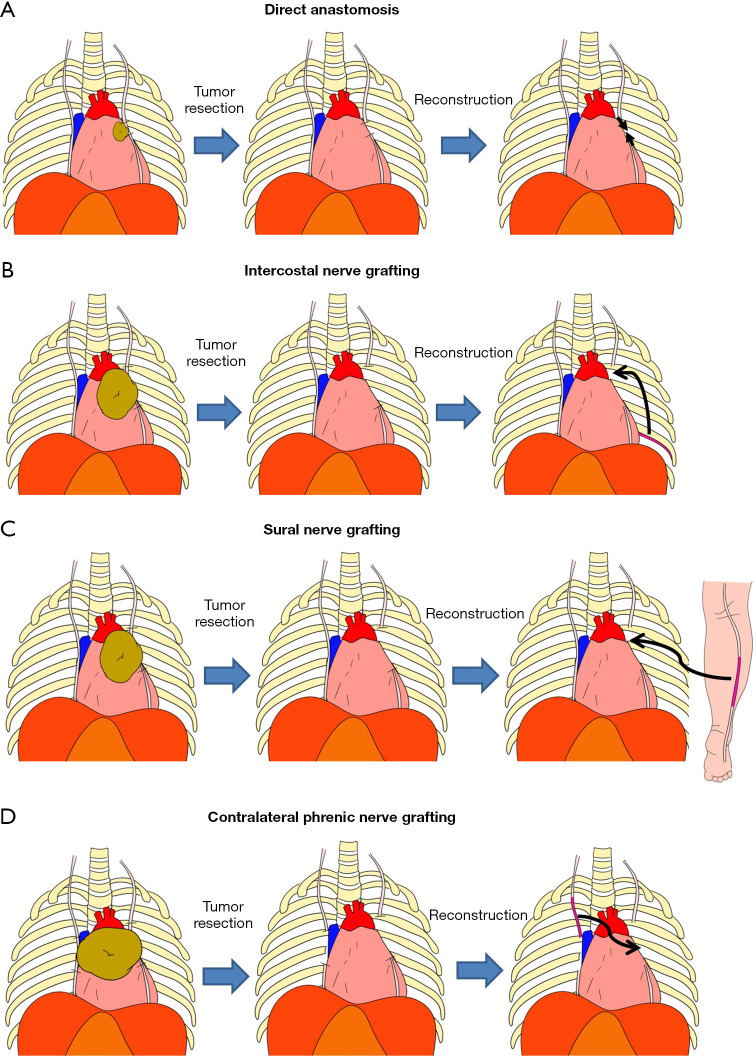
Key content and findings: Phrenic nerve reconstruction can be performed either immediately after nerve resection or as a delayed procedure. Immediate reconstruction, especially when conducted concurrently with tumor resection, has been shown to promote optimal nerve regeneration and functional recovery. In contrast, delayed reconstruction is generally associated with greater technical challenges and less predictable outcomes. Direct anastomosis is preferable when feasible; however, nerve grafting is often required due to insufficient residual nerve length to achieve a tension-free repair. Among graft options, the intercostal nerve is favorable due to its anatomical proximity and minimal additional surgical burden, whereas the use of other nerves, such as the sural nerve, requires an additional incision at a separate site, which may be less desirable. Successful reconstruction can also be achieved using minimally invasive approaches such as video-assisted thoracoscopic surgery (VATS) and robotic-assisted thoracoscopic surgery (RATS). Notably, the additional time required for reconstruction in minimally invasive procedures is manageable and does not significantly affect patient outcomes.
Conclusions: Immediate phrenic nerve reconstruction, either by direct suturing or intercostal nerve grafting, is a feasible and effective method for preserving respiratory function. The ability to perform reconstruction using minimally invasive techniques further supports its clinical adoption. Given its advantages in functional recovery and its relatively low additional surgical burden, phrenic nerve resection followed by immediate reconstruction may be considered in most cases involving phrenic nerve invasion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


