Thomas F Imperiale, Michael Cheng, Melissa R Thomas, Marianne S Matthias
{"title":"A qualitative study of a new metric for estimating early-onset colorectal cancer risk in male veterans: \"Colon Age\".","authors":"Thomas F Imperiale, Michael Cheng, Melissa R Thomas, Marianne S Matthias","doi":"10.1186/s12875-025-02854-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In several Western nations, cancers of the colon and rectum have been steadily increasing in persons younger than age 50. Although the age at which to begin colorectal cancer (CRC) screening in the U.S. was lowered to 45 years in 2018, uptake of screening in persons aged 45-49 has been slow. Based on risk factors for CRC prior to age 50 and population-based CRC prevalence data, we previously defined a new metric for estimating the risk of CRC prior to age 50 called \"Colon Age\". The objective of this study was to obtain qualitative data on the acceptance, feasibility, and clinical utility of this metric from patients and primary care providers.</p><p><strong>Methods: </strong>With permission from their providers, we recruited a convenience sample of average-risk male patients 35-49 years of age during their primary care appointment. Primary care providers were recruited through email invitation. Following informed consent, two interviewers conducted semi-structured qualitative interviews with participants. Interviews were conducted until saturation was reached. Interviewers were not involved in the tool's development. The audio-recorded interviews were transcribed, de-identified, and analyzed using the constant comparison method.</p><p><strong>Results: </strong>Thirty-one (23 male Veteran patients, 8 primary care providers) interviews were conducted. Patients (mean age 47 years, 100% male) expressed willingness to follow screening recommendations from their provider, although most were unaware of other screening options beyond colonoscopy. Overall, patients expressed acceptance of the Colon Age concept and tool, finding it easy to understand, helpful for staying informed of their health, and a way to empower themselves in their screening decisions. Providers (mean age 53 years; 50% female) also found the tool acceptable, commenting on its usefulness for starting screening conversations with patients and improving screening uptake. Providers questioned the tool's time commitment, consistency with practice guidelines, and the process of tool development.</p><p><strong>Conclusions: </strong>In this age of precision medicine, the Colon Age tool-despite some limitations-appears to be useful to patients and providers in individualizing risk for CRC and may improve uptake of screening in persons younger than age 50.</p>","PeriodicalId":72428,"journal":{"name":"BMC primary care","volume":"26 1","pages":"226"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12265148/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC primary care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12875-025-02854-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In several Western nations, cancers of the colon and rectum have been steadily increasing in persons younger than age 50. Although the age at which to begin colorectal cancer (CRC) screening in the U.S. was lowered to 45 years in 2018, uptake of screening in persons aged 45-49 has been slow. Based on risk factors for CRC prior to age 50 and population-based CRC prevalence data, we previously defined a new metric for estimating the risk of CRC prior to age 50 called "Colon Age". The objective of this study was to obtain qualitative data on the acceptance, feasibility, and clinical utility of this metric from patients and primary care providers.
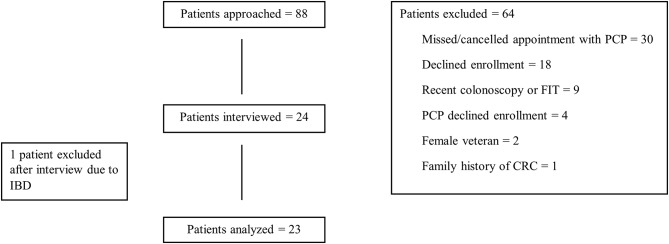
Methods: With permission from their providers, we recruited a convenience sample of average-risk male patients 35-49 years of age during their primary care appointment. Primary care providers were recruited through email invitation. Following informed consent, two interviewers conducted semi-structured qualitative interviews with participants. Interviews were conducted until saturation was reached. Interviewers were not involved in the tool's development. The audio-recorded interviews were transcribed, de-identified, and analyzed using the constant comparison method.
Results: Thirty-one (23 male Veteran patients, 8 primary care providers) interviews were conducted. Patients (mean age 47 years, 100% male) expressed willingness to follow screening recommendations from their provider, although most were unaware of other screening options beyond colonoscopy. Overall, patients expressed acceptance of the Colon Age concept and tool, finding it easy to understand, helpful for staying informed of their health, and a way to empower themselves in their screening decisions. Providers (mean age 53 years; 50% female) also found the tool acceptable, commenting on its usefulness for starting screening conversations with patients and improving screening uptake. Providers questioned the tool's time commitment, consistency with practice guidelines, and the process of tool development.
Conclusions: In this age of precision medicine, the Colon Age tool-despite some limitations-appears to be useful to patients and providers in individualizing risk for CRC and may improve uptake of screening in persons younger than age 50.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


