{"title":"Association of Presenting Complaint at Triage with 72-h Mortality and Intensive Care Admission.","authors":"Niraj Rauniyar, Ankit Kumar Sahu, Bharath Gopinath, Akshay Kumar, Nayer Jamshed, Meera Ekka, Prakash Ranjan Mishra, Sanjeev Bhoi, Tej Prakash Sinha, Gaurav Rajwanshi","doi":"10.4103/jets.jets_127_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Triage is a critical process in prioritizing patients based on acuity to ensure timely care. Patients arrive at the emergency department (ED) with complaints, not diagnoses. High-risk patients are identified based on history, vital signs, mechanism of injury in trauma, and clinical findings. Chief complaints in the ED may suggest acuity independent of other clinical parameters. The objective of this study was to identify high-risk chief complaints associated with intensive care unit (ICU) admission or mortality within 72 h of ED presentation. We also characterized the chief complaints by frequency and evaluated the accuracy of the All India Institute of Medical Sciences Triage Protocol (ATP) in conjunction with high-risk complaints for predicting mortality.</p><p><strong>Methods: </strong>This prospective observational study was conducted at AIIMS, New Delhi, from March 2021 to October 2023, including 1225 patients. Inclusion criteria covered all patients older than 16 years presenting to the ED, excluding cardiac arrest cases, pregnancy-related complications, and individuals declared dead on arrival. Data were collected using predesigned proformas. Univariate and multivariate logistic regression analyses identified high-risk chief complaints.</p><p><strong>Results: </strong>Of the 1754 patients screened, 1225 were included in the analysis. Thirty-four complaints were identified, with six deemed high risk. Specific complaints such as shortness of breath (odds ratio [OR] 43.691, 95% confidence interval [CI] 20.033-95.291, <i>P</i> = 0.001), altered mental status (OR: 6.243, 95% CI: 3.282-11.876, <i>P</i> < 0.001), hematemesis (OR: 3.88, 95% CI: 2.019-7.454, <i>P</i> < 0.001), fall from height (OR: 3.875, 95% CI: 1.874-8.014, <i>P</i> < 0.001), weakness of one side (OR: 3.159, 95% CI: 1.656-6.024, <i>P</i> < 0.001), and chest pain (OR: 1.784, 95% CI: 1.22-3.209, <i>P</i> = 0.043) were significantly associated with adverse outcomes (mortality or ICU admission) at 72 h, even after adjusting for age, gender, and comorbidities. Incorporating high-risk complaints into the ATP triage system increased predictive value (OR 3.12 vs. 7.14).</p><p><strong>Conclusion: </strong>Our findings highlight specific chief complaints as valuable indicators for the early identification of patients at risk of 72-h mortality or ICU admission in the ED. Early identification of high-risk patients can enhance early resuscitation, timely referral to higher-level care, and improve patient outcomes.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"18 2","pages":"62-68"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258527/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_127_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Triage is a critical process in prioritizing patients based on acuity to ensure timely care. Patients arrive at the emergency department (ED) with complaints, not diagnoses. High-risk patients are identified based on history, vital signs, mechanism of injury in trauma, and clinical findings. Chief complaints in the ED may suggest acuity independent of other clinical parameters. The objective of this study was to identify high-risk chief complaints associated with intensive care unit (ICU) admission or mortality within 72 h of ED presentation. We also characterized the chief complaints by frequency and evaluated the accuracy of the All India Institute of Medical Sciences Triage Protocol (ATP) in conjunction with high-risk complaints for predicting mortality.
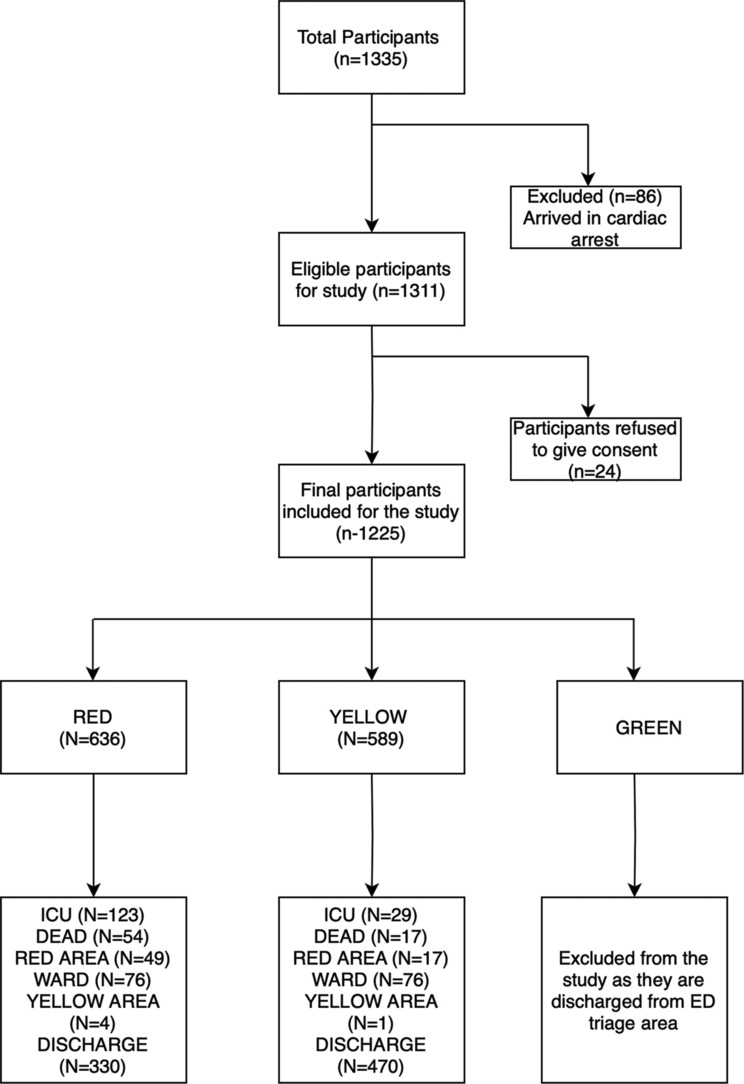
Methods: This prospective observational study was conducted at AIIMS, New Delhi, from March 2021 to October 2023, including 1225 patients. Inclusion criteria covered all patients older than 16 years presenting to the ED, excluding cardiac arrest cases, pregnancy-related complications, and individuals declared dead on arrival. Data were collected using predesigned proformas. Univariate and multivariate logistic regression analyses identified high-risk chief complaints.
Results: Of the 1754 patients screened, 1225 were included in the analysis. Thirty-four complaints were identified, with six deemed high risk. Specific complaints such as shortness of breath (odds ratio [OR] 43.691, 95% confidence interval [CI] 20.033-95.291, P = 0.001), altered mental status (OR: 6.243, 95% CI: 3.282-11.876, P < 0.001), hematemesis (OR: 3.88, 95% CI: 2.019-7.454, P < 0.001), fall from height (OR: 3.875, 95% CI: 1.874-8.014, P < 0.001), weakness of one side (OR: 3.159, 95% CI: 1.656-6.024, P < 0.001), and chest pain (OR: 1.784, 95% CI: 1.22-3.209, P = 0.043) were significantly associated with adverse outcomes (mortality or ICU admission) at 72 h, even after adjusting for age, gender, and comorbidities. Incorporating high-risk complaints into the ATP triage system increased predictive value (OR 3.12 vs. 7.14).
Conclusion: Our findings highlight specific chief complaints as valuable indicators for the early identification of patients at risk of 72-h mortality or ICU admission in the ED. Early identification of high-risk patients can enhance early resuscitation, timely referral to higher-level care, and improve patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


