Elena Céspedes-Martínez, Virginia Robles-Alonso, Xavier Serra-Ruiz, Claudia Herrera-De Guise, Luis Mayorga-Ayala, Sonia García-García, María Larrosa-García, Francesc Casellas, Natalia Borruel
{"title":"Dashboard-Guided Anti-TNF Induction: An Effective Strategy to Minimize Immunogenicity While Avoiding Immunomodulators-A Single-Center Cohort Study.","authors":"Elena Céspedes-Martínez, Virginia Robles-Alonso, Xavier Serra-Ruiz, Claudia Herrera-De Guise, Luis Mayorga-Ayala, Sonia García-García, María Larrosa-García, Francesc Casellas, Natalia Borruel","doi":"10.1093/crocol/otaf023","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Proactive therapeutic drug monitoring facilitates early dose optimization to prevent primary and secondary failure to antitumor necrosis factor (TNF). We aimed to investigate the impact of dashboard-guided induction dosing strategy on anti-TNF durability and immunogenicity.</p><p><strong>Methods: </strong>We conducted a single-center cohort analysis of patients with Crohn's disease (CD) and Ulcerative colitis (UC) who initiated treatment with infliximab or adalimumab between January 2020 and March 2023. Induction was prospectively personalized using a pharmacokinetic model-guided dosing strategy, with drug measurements at week 2, 6, and 14, and the first dose adjustment occurred in week 4. Data were recorded retrospectively. We assessed treatment durability, pharmacokinetic outcomes, clinical remission (CR), and endoscopic remission (ER), at both weeks 24 and 56. Multivariate analysis and Kaplan-Meier curves were used to compare outcomes.</p><p><strong>Results: </strong>We enrolled 147 patients (92 CD /55 UC). Anti-TNF drug survival probability was 85.00% after a year. Seventy-seven percent of patients were prescribed an intensified dose in the first year, which was associated with improved drug durability. Only 1 patient out of 147 developed antibodies to adalimumab, none to infliximab. After 24 and 52 weeks of treatment 92.5% (136/147) and 72.78% (107/147) of patients achieved CR, respectively. ER was observed in 59.39% (79/133) of patients. The use of immunomodulators or carriage of HLA DQA1*05 variant was not associated with adverse treatment or pharmacokinetic outcomes.</p><p><strong>Conclusions: </strong>Optimizing anti-TNF induction with a dashboard-guide dosing strategy proves to be a valuable approach to enhance treatment durability and clinical outcomes in inflammatory bowel disease patients. Immunogenicity appears to be mitigated by the model, which even mitigates the impact of immunomodulators and overcomes HLA DQA1*05 effect.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 3","pages":"otaf023"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12260160/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Proactive therapeutic drug monitoring facilitates early dose optimization to prevent primary and secondary failure to antitumor necrosis factor (TNF). We aimed to investigate the impact of dashboard-guided induction dosing strategy on anti-TNF durability and immunogenicity.
Methods: We conducted a single-center cohort analysis of patients with Crohn's disease (CD) and Ulcerative colitis (UC) who initiated treatment with infliximab or adalimumab between January 2020 and March 2023. Induction was prospectively personalized using a pharmacokinetic model-guided dosing strategy, with drug measurements at week 2, 6, and 14, and the first dose adjustment occurred in week 4. Data were recorded retrospectively. We assessed treatment durability, pharmacokinetic outcomes, clinical remission (CR), and endoscopic remission (ER), at both weeks 24 and 56. Multivariate analysis and Kaplan-Meier curves were used to compare outcomes.
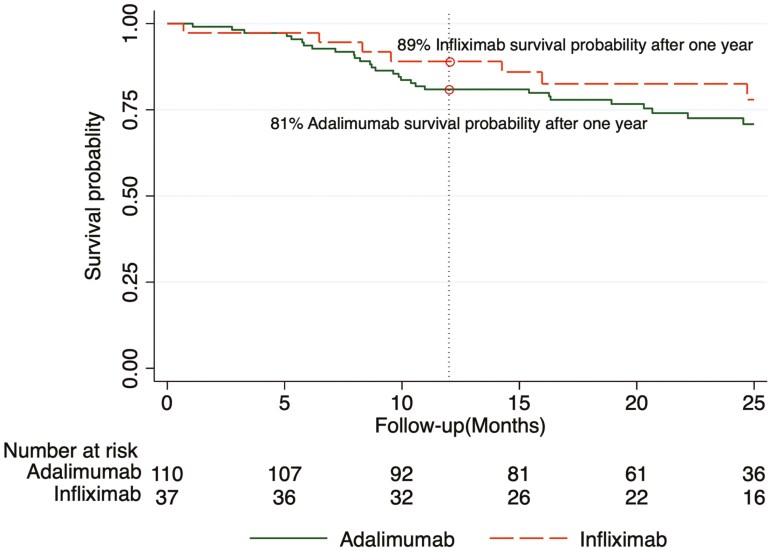
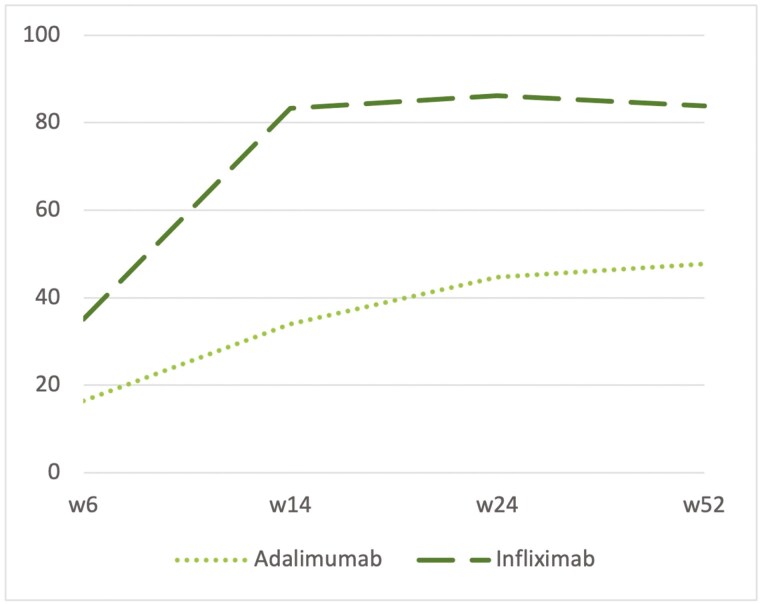
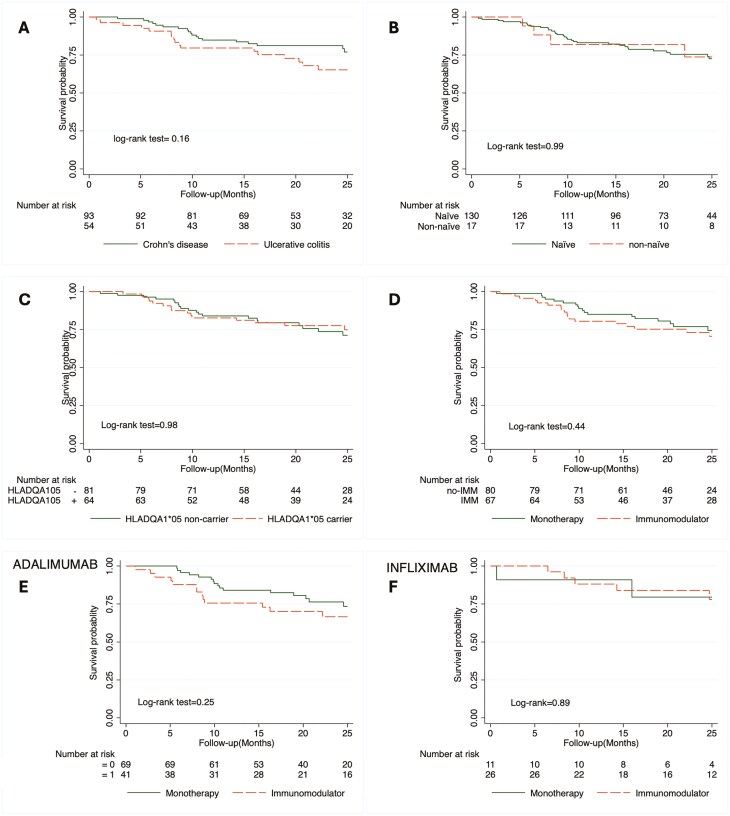
Results: We enrolled 147 patients (92 CD /55 UC). Anti-TNF drug survival probability was 85.00% after a year. Seventy-seven percent of patients were prescribed an intensified dose in the first year, which was associated with improved drug durability. Only 1 patient out of 147 developed antibodies to adalimumab, none to infliximab. After 24 and 52 weeks of treatment 92.5% (136/147) and 72.78% (107/147) of patients achieved CR, respectively. ER was observed in 59.39% (79/133) of patients. The use of immunomodulators or carriage of HLA DQA1*05 variant was not associated with adverse treatment or pharmacokinetic outcomes.
Conclusions: Optimizing anti-TNF induction with a dashboard-guide dosing strategy proves to be a valuable approach to enhance treatment durability and clinical outcomes in inflammatory bowel disease patients. Immunogenicity appears to be mitigated by the model, which even mitigates the impact of immunomodulators and overcomes HLA DQA1*05 effect.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


