{"title":"Clinical outcomes of endoscopic ultrasound-guided hepaticogastrostomy-based internal drainage for unresectable malignant hilar biliary obstruction: a comprehensive evaluation with malignant distal biliary obstruction.","authors":"Daiki Yamashige, Susumu Hijioka, Yoshikuni Nagashio, Shota Harai, Yasuhiro Komori, Aoi Kita, Masaru Kuwada, Soma Fukuda, Shin Yagi, Kohei Okamoto, Daiki Agarie, Shunsuke Sugawara, Miyuki Sone, Yutaka Saito, Takuji Okusaka","doi":"10.1177/17562848251356099","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) may not provide adequate drainage for patients with malignant hilar biliary obstruction (MHBO). Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is a salvage method for malignant distal biliary obstruction (MDBO); however, its effectiveness for MHBO remains unclear.</p><p><strong>Objectives: </strong>We aimed to evaluate the short- and long-term outcomes of EUS-HGS for MHBO.</p><p><strong>Design: </strong>This was a single-center retrospective cohort study.</p><p><strong>Methods: </strong>Unresectable patients who underwent initial EUS-HGS because of ERCP failure were recruited. Distal biliary stenosis or Bismuth types I and II-IV were defined as MDBO and MHBO, respectively. We defined EUS-HGS for MDBO as the control and analyzed the outcomes for MHBO.</p><p><strong>Results: </strong>The MDBO group (<i>n</i> = 208) was treated using EUS-HGS alone. In the MHBO group (<i>n</i> = 63), EUS-HGS alone (unilateral drainage, <i>n</i> = 26), EUS-HGS with bridging (EUS-HGSB, bilateral drainage, <i>n</i> = 21), and ERCP + EUS-HGS (bilateral drainage, <i>n</i> = 16) were performed. In EUS-HGS (MDBO), EUS-HGS (MHBO), EUS-HGSB, and ERCP + EUS-HGS, the technical success rates were 98.6%, 96.3%, 95.5%, and 94.1%; clinical success rates were 88.5%, 76.9%, 85.7%, and 75.0%; adverse event rates were 19.7%, 15.4%, 9.5%, and 25.0%; and non-recurrent biliary obstruction (RBO) rates at 180 days were 45.5%, 19.8%, 61.9%, and 68.4%, respectively. In multivariate analysis of the MHBO group, EUS-HGSB tended to have a lower risk of RBO (adjusted hazard ratio (aHR), 0.39; <i>p</i> = 0.09), and ERCP + EUS-HGS showed a significantly lower risk (aHR, 0.25; <i>p</i> = 0.03) compared to EUS-HGS alone (unilateral drainage).</p><p><strong>Conclusion: </strong>ERCP + EUS-HGS followed by EUS-HGSB, providing bilateral drainage, can offer preferred palliation for MHBO. These drainages may serve as potential salvage options in the management of MHBO.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251356099"},"PeriodicalIF":3.4000,"publicationDate":"2025-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12256750/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251356099","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endoscopic retrograde cholangiopancreatography (ERCP) may not provide adequate drainage for patients with malignant hilar biliary obstruction (MHBO). Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is a salvage method for malignant distal biliary obstruction (MDBO); however, its effectiveness for MHBO remains unclear.
Objectives: We aimed to evaluate the short- and long-term outcomes of EUS-HGS for MHBO.
Design: This was a single-center retrospective cohort study.
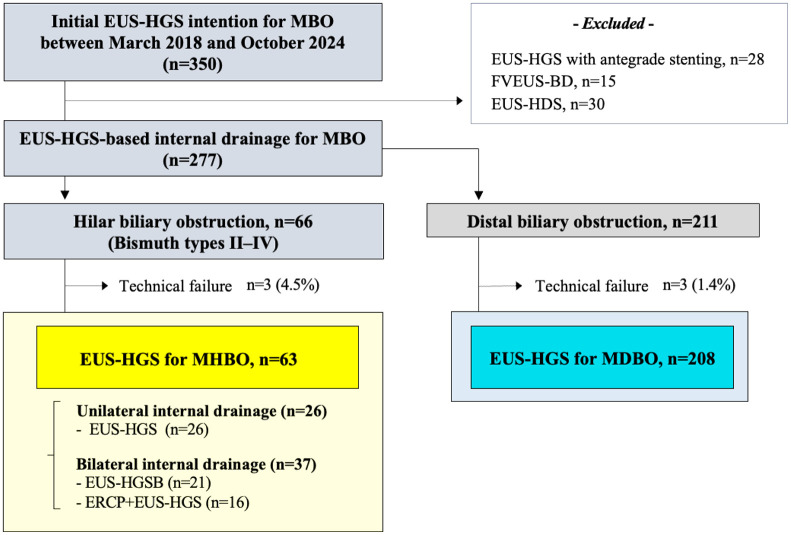
Methods: Unresectable patients who underwent initial EUS-HGS because of ERCP failure were recruited. Distal biliary stenosis or Bismuth types I and II-IV were defined as MDBO and MHBO, respectively. We defined EUS-HGS for MDBO as the control and analyzed the outcomes for MHBO.
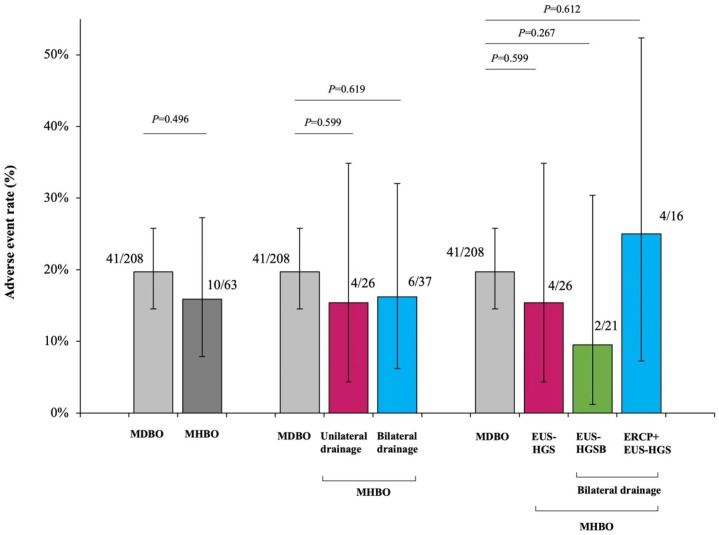
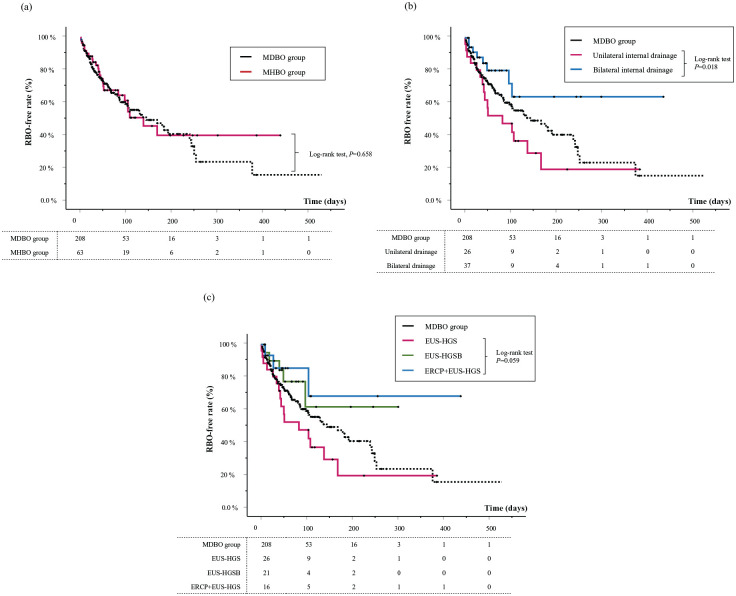
Results: The MDBO group (n = 208) was treated using EUS-HGS alone. In the MHBO group (n = 63), EUS-HGS alone (unilateral drainage, n = 26), EUS-HGS with bridging (EUS-HGSB, bilateral drainage, n = 21), and ERCP + EUS-HGS (bilateral drainage, n = 16) were performed. In EUS-HGS (MDBO), EUS-HGS (MHBO), EUS-HGSB, and ERCP + EUS-HGS, the technical success rates were 98.6%, 96.3%, 95.5%, and 94.1%; clinical success rates were 88.5%, 76.9%, 85.7%, and 75.0%; adverse event rates were 19.7%, 15.4%, 9.5%, and 25.0%; and non-recurrent biliary obstruction (RBO) rates at 180 days were 45.5%, 19.8%, 61.9%, and 68.4%, respectively. In multivariate analysis of the MHBO group, EUS-HGSB tended to have a lower risk of RBO (adjusted hazard ratio (aHR), 0.39; p = 0.09), and ERCP + EUS-HGS showed a significantly lower risk (aHR, 0.25; p = 0.03) compared to EUS-HGS alone (unilateral drainage).
Conclusion: ERCP + EUS-HGS followed by EUS-HGSB, providing bilateral drainage, can offer preferred palliation for MHBO. These drainages may serve as potential salvage options in the management of MHBO.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


