Massimo Iavarone, Eleonora Alimenti, Lorenzo Canova, Mariangela Bruccoleri, Barbara Antonelli, Anna Maria Ierardi, Angelo Sangiovanni, Giuseppe Cabibbo, Annalisa De Silvestri, Lucio Caccamo, Gianpaolo Carrafiello, Pietro Lampertico
{"title":"The impact of BCLC recommendations on survival for patients with hepatocellular carcinoma.","authors":"Massimo Iavarone, Eleonora Alimenti, Lorenzo Canova, Mariangela Bruccoleri, Barbara Antonelli, Anna Maria Ierardi, Angelo Sangiovanni, Giuseppe Cabibbo, Annalisa De Silvestri, Lucio Caccamo, Gianpaolo Carrafiello, Pietro Lampertico","doi":"10.1097/HC9.0000000000000750","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Barcelona Clinic Liver Cancer (BCLC) system for HCC was updated in 2022. The aim of the study was to assess the suitability and impact on overall survival (OS) of BCLC_2022, along with \"clinical decision-making\" (CDM), using BCLC_2018 as a benchmark.</p><p><strong>Methods: </strong>We retrospectively evaluated 798 patients with de novo HCC followed prospectively from 2006 to 2022: 187 in BCLC 0, 371 in A, 132 in B, 87 in C, and 21 in D, all managed by a multidisciplinary team. Patients were followed until death or at the end of the follow-up period in December 2022.</p><p><strong>Results: </strong>The suitability of the algorithm increased from 51% for BCLC_2018 to 69% for BCLC_2022 (p<0.001). Among those treated with the newly introduced \"lower priority options,\" 22% were in BCLC 0 and 37% in A, showing lower rates of complete response (CR) and shorter OS compared to first-line treatments. In BCLC 0 and A, CDM was associated with a significant decrease in \"downward stage migration\" with BCLC_2022 (from 33% to 16%, p<0.001). Conversely, in BCLC B and C, \"upward stage migration\" correlated with higher CR rates and longer OS [63 (36-72) vs. 28 (18-44) months, p=0.003 in BCLC B; 21 (15-44) vs. 11 (4-25) months, p<0.001 in BCLC C]. Independent predictors of mortality included AFP >200 ng/mL, Child-Pugh score C, advanced BCLC stage, and noncurative treatment.</p><p><strong>Conclusions: </strong>BCLC_2022 and CDM provide greater flexibility in clinical practice without adversely affecting patient survival. Access to curative treatments improves the outcomes of selected patients in all stages.</p>","PeriodicalId":12978,"journal":{"name":"Hepatology Communications","volume":"9 8","pages":""},"PeriodicalIF":5.6000,"publicationDate":"2025-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12263035/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology Communications","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/HC9.0000000000000750","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
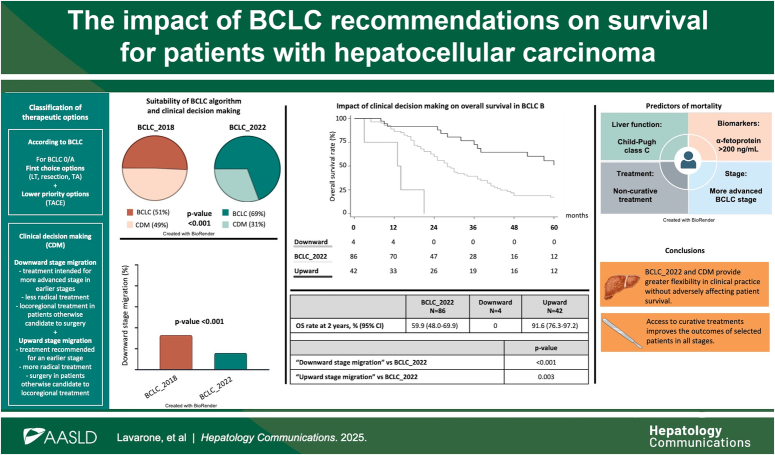
Background: The Barcelona Clinic Liver Cancer (BCLC) system for HCC was updated in 2022. The aim of the study was to assess the suitability and impact on overall survival (OS) of BCLC_2022, along with "clinical decision-making" (CDM), using BCLC_2018 as a benchmark.
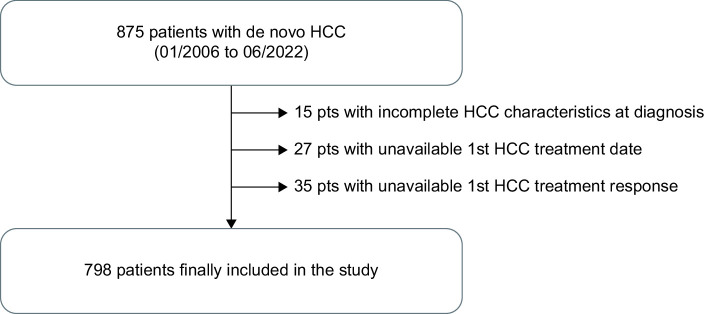
Methods: We retrospectively evaluated 798 patients with de novo HCC followed prospectively from 2006 to 2022: 187 in BCLC 0, 371 in A, 132 in B, 87 in C, and 21 in D, all managed by a multidisciplinary team. Patients were followed until death or at the end of the follow-up period in December 2022.
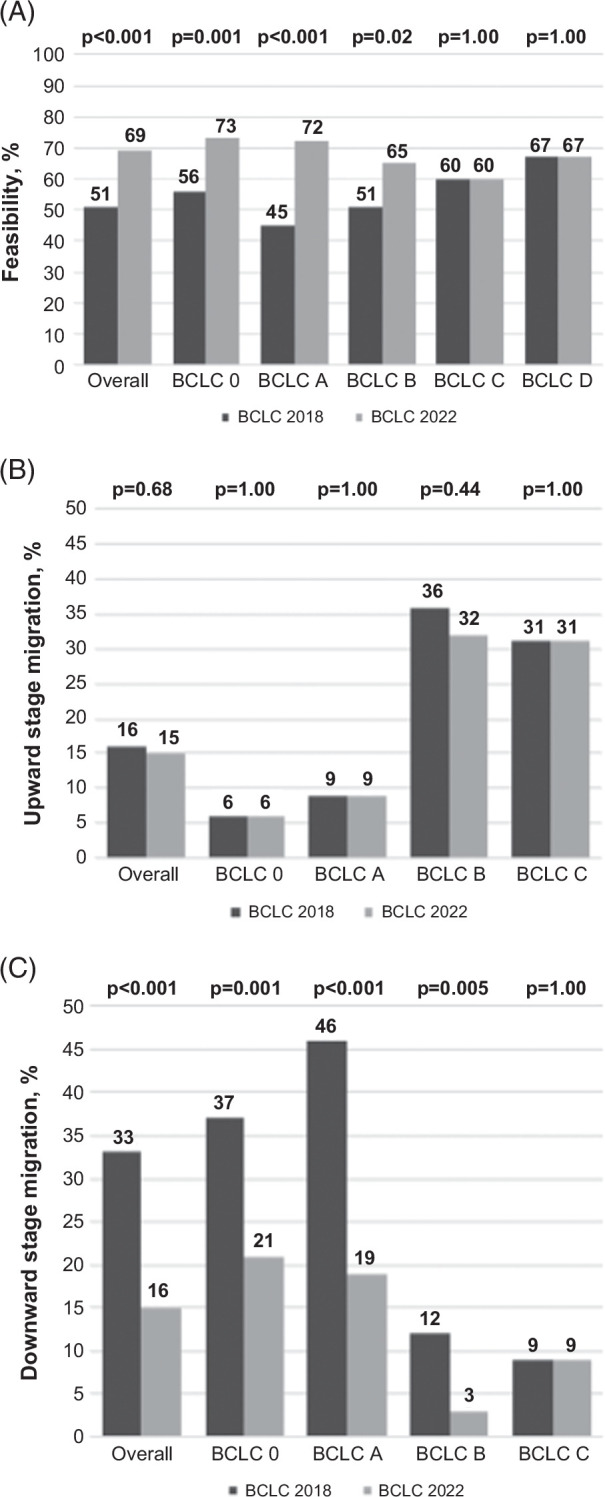
Results: The suitability of the algorithm increased from 51% for BCLC_2018 to 69% for BCLC_2022 (p<0.001). Among those treated with the newly introduced "lower priority options," 22% were in BCLC 0 and 37% in A, showing lower rates of complete response (CR) and shorter OS compared to first-line treatments. In BCLC 0 and A, CDM was associated with a significant decrease in "downward stage migration" with BCLC_2022 (from 33% to 16%, p<0.001). Conversely, in BCLC B and C, "upward stage migration" correlated with higher CR rates and longer OS [63 (36-72) vs. 28 (18-44) months, p=0.003 in BCLC B; 21 (15-44) vs. 11 (4-25) months, p<0.001 in BCLC C]. Independent predictors of mortality included AFP >200 ng/mL, Child-Pugh score C, advanced BCLC stage, and noncurative treatment.
Conclusions: BCLC_2022 and CDM provide greater flexibility in clinical practice without adversely affecting patient survival. Access to curative treatments improves the outcomes of selected patients in all stages.
期刊介绍:
Hepatology Communications is a peer-reviewed, online-only, open access journal for fast dissemination of high quality basic, translational, and clinical research in hepatology. Hepatology Communications maintains high standard and rigorous peer review. Because of its open access nature, authors retain the copyright to their works, all articles are immediately available and free to read and share, and it is fully compliant with funder and institutional mandates. The journal is committed to fast publication and author satisfaction.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


