Amit Prajapati, Yubaraj Sharma, Suman Thapa, Sadina Devkota
{"title":"DECAF Score in Predicting Outcomes of Acute Exacerbation of Chronic Obstructive Pulmonary Disease: An Observational Study.","authors":"Amit Prajapati, Yubaraj Sharma, Suman Thapa, Sadina Devkota","doi":"10.31729/jnma.8903","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) can often lead to hospital admission and has the potential to be fatal. Lack of prognostic research in exacerbation requiring hospitalization that can accurately predict inhospital mortality is a challenge. This study aims to assess value of the DECAF (Dyspnea, Eosinopenia, Consolidation, Acidemia and Atrial fibrillation) score as a clinical prediction tool for inhospital mortality, need of intensive care unit (ICU) stay and risk stratification in patients with Acute exacerbation of chronic obstructive pulmonary disease.</p><p><strong>Methods: </strong>This is an observational cross-section, hospital based study conducted from April 2022 to February 2023 at a tertiary care centre. The patients admitted with the diagnosis of acute exacerbation of chronic obstructive pulmonary disease were included in the study and their DECAF score were calculated. Patients were followed up during hospital stay and their outcome were recorded. The prognostic value of DECAF score was assessed by area under receiver operator characterstics curve.</p><p><strong>Results: </strong>There were 83 patients enrolled in the study out of which 13 (15.66%) died in the hospital and 20 (24.09%) required ICU stay. The area under receiver operator characteristic curve value for mortality owas 0.89 and that for intensive care unit stay was 0.84.</p><p><strong>Conclusions: </strong>This study shows that DECAF score is a good predictor of inhospital mortality and ICU admission.</p>","PeriodicalId":520657,"journal":{"name":"JNMA; journal of the Nepal Medical Association","volume":"63 283","pages":"144-148"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122275/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNMA; journal of the Nepal Medical Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31729/jnma.8903","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) can often lead to hospital admission and has the potential to be fatal. Lack of prognostic research in exacerbation requiring hospitalization that can accurately predict inhospital mortality is a challenge. This study aims to assess value of the DECAF (Dyspnea, Eosinopenia, Consolidation, Acidemia and Atrial fibrillation) score as a clinical prediction tool for inhospital mortality, need of intensive care unit (ICU) stay and risk stratification in patients with Acute exacerbation of chronic obstructive pulmonary disease.
Methods: This is an observational cross-section, hospital based study conducted from April 2022 to February 2023 at a tertiary care centre. The patients admitted with the diagnosis of acute exacerbation of chronic obstructive pulmonary disease were included in the study and their DECAF score were calculated. Patients were followed up during hospital stay and their outcome were recorded. The prognostic value of DECAF score was assessed by area under receiver operator characterstics curve.
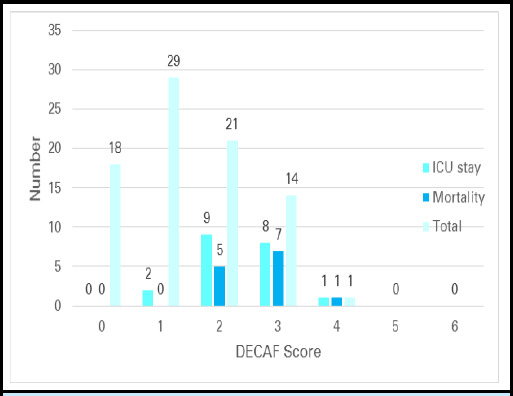
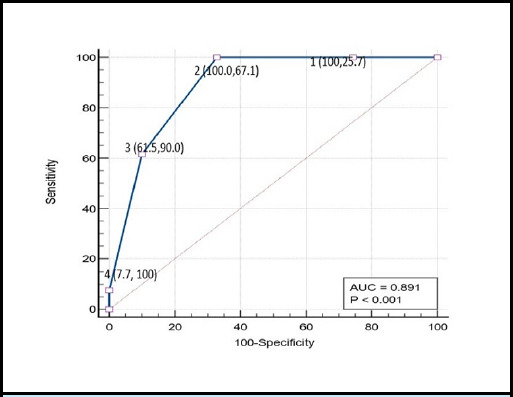
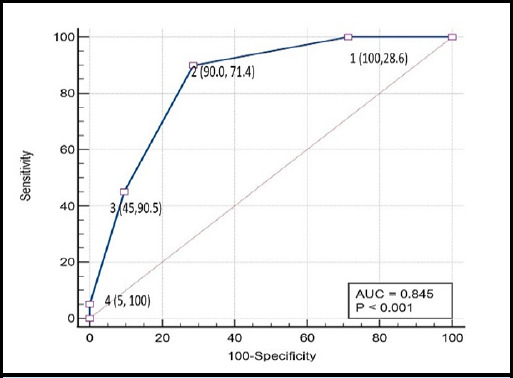
Results: There were 83 patients enrolled in the study out of which 13 (15.66%) died in the hospital and 20 (24.09%) required ICU stay. The area under receiver operator characteristic curve value for mortality owas 0.89 and that for intensive care unit stay was 0.84.
Conclusions: This study shows that DECAF score is a good predictor of inhospital mortality and ICU admission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


