Endometrial compaction shows no association with improved pregnancy outcomes in hormonal replacement frozen-thawed embryo transfer: an analysis of over 16 000 cases.
Peipei Pan, Chang Liu, Shiyi Lin, Haiqing Wang, Xia Chen, Haiyan Yang, Xuefeng Huang, Huan Zhang, Yili Teng
{"title":"Endometrial compaction shows no association with improved pregnancy outcomes in hormonal replacement frozen-thawed embryo transfer: an analysis of over 16 000 cases.","authors":"Peipei Pan, Chang Liu, Shiyi Lin, Haiqing Wang, Xia Chen, Haiyan Yang, Xuefeng Huang, Huan Zhang, Yili Teng","doi":"10.1093/hropen/hoaf039","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Is there an association between changes in endometrial thickness (EMT) following progesterone administration and pregnancy outcomes in frozen-thawed embryo transfers (FETs) at Day 3 (D3) and blastocyst stages?</p><p><strong>Summary answer: </strong>Endometrial compaction is not associated with better pregnancy outcomes.</p><p><strong>What is known already: </strong>Previous studies have shown conflicting results on the impact of EMT changes on FET outcomes.</p><p><strong>Study design size duration: </strong>This study was a single-center retrospective cohort analysis of FETs from 1 January 2018 to 31 December 2022. A total of 9390 D3 FETs and 7063 blastocyst FETs were included during this period.</p><p><strong>Participants/materials setting methods: </strong>D3 FETs and blastocyst FETs were divided into three groups: compaction group, non-change group, and expansion group. The impact of EMT changes after progesterone administration on HCG-positive, pregnancy, ongoing pregnancy, live birth, and pregnancy loss rates were analyzed for D3 and blastocyst FETs. EMT on the progesterone administration day (defined as EMT1) and on embryo transfer (ET)day (defined as EMT2) was measured exclusively by transvaginal ultrasound. Inverse probability weighting (IPW) and stratified logistic regressions were conducted to reduce the effects of confounding factors.</p><p><strong>Main results and the role of chance: </strong>After IPW adjustment, in D3 FETs, women with compacted endometrium had the lowest HCG-positive rates (<i>P </i>= 0.012), clinical pregnancy rates (<i>P </i>< 0.001), ongoing pregnancy rates (<i>P </i>< 0.001), and live birth rates (LBRs) (<i>P </i>< 0.001) among the three groups. Among HCG-positive cases, the compaction group had the highest ectopic pregnancy rates (3.5% vs 2.6% vs 1.6%; <i>P </i>= 0.015) and the lowest LBRs (65.8% vs 68.3% vs 71.4%; <i>P </i>= 0.018). Univariate logistic regressions found that LBRs were weakly associated with compacted endometrium [odds ratio (OR) 0.831, 95% CI: 0.696-0.993]. Logistic regressions with IPW revealed that the compaction group was not associated with higher odds of pregnancy outcomes, including HCG positive, clinical pregnancy, ongoing pregnancy, ongoing pregnancy, and live births compared to the non-change group. In contrast, the expansion group was associated with higher odds of live birth per ETs (OR 1.166, 95% CI: 1.070-1.271; <i>P </i>= 0.001), and live birth per HCG-positive cases (OR 1.160, 95% CI: 1.028-1.309; <i>P </i>= 0.016). In blastocyst FETs, women with compacted endometrium had the lowest HCG-positive rates (<i>P </i>= 0.001) and clinical pregnancy rates (<i>P </i>= 0.031). Logistic regressions with IPW adjustment found that compaction group was associated with lower odds of HCG positive (OR 0.813, 95% CI: 0.668-0.989, <i>P </i>= 0.039) compared to the non-change group. Additionally, LBRs increased with the rising change ratios of EMT after progesterone administration, but within a certain range (30% in D3 FETs and 50% in blastocyst FETs).</p><p><strong>Limitations reasons for caution: </strong>This study only included retrospective analyses of untested embryos for FETs.</p><p><strong>Wider implications of the findings: </strong>Endometrial expansion in D3 FETs exhibited a positive association with improved LBRs, but not in blastocyst FETs. These findings suggest that embryo developmental stage-specific endometrial preparation protocols may enhance assisted reproductive outcomes.</p><p><strong>Study funding/competing interests: </strong>This study was supported by National Natural Science Foundation of China (82201856), Basic Scientific Research project of Wenzhou Science and Technology Bureau (Y20220006), Wenzhou Key Laboratory of Reproduction and Genetics (2022HZSY0051), and Clinical Technology International Exchange Project of Zhejiang Provincial Medical Institutions. The authors have no conflicts of interest to declare.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 3","pages":"hoaf039"},"PeriodicalIF":11.1000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12255888/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: Is there an association between changes in endometrial thickness (EMT) following progesterone administration and pregnancy outcomes in frozen-thawed embryo transfers (FETs) at Day 3 (D3) and blastocyst stages?
Summary answer: Endometrial compaction is not associated with better pregnancy outcomes.
What is known already: Previous studies have shown conflicting results on the impact of EMT changes on FET outcomes.
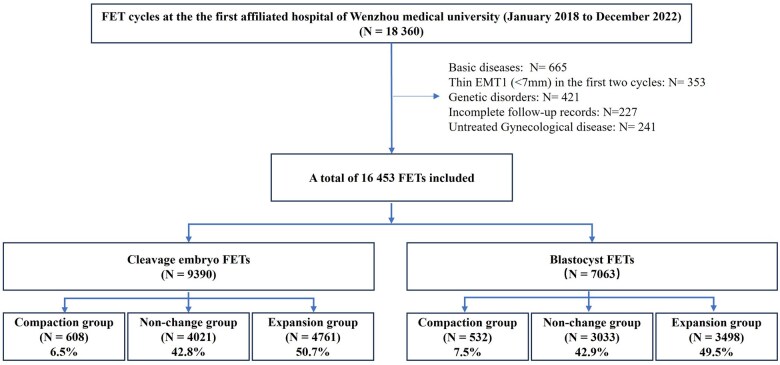
Study design size duration: This study was a single-center retrospective cohort analysis of FETs from 1 January 2018 to 31 December 2022. A total of 9390 D3 FETs and 7063 blastocyst FETs were included during this period.
Participants/materials setting methods: D3 FETs and blastocyst FETs were divided into three groups: compaction group, non-change group, and expansion group. The impact of EMT changes after progesterone administration on HCG-positive, pregnancy, ongoing pregnancy, live birth, and pregnancy loss rates were analyzed for D3 and blastocyst FETs. EMT on the progesterone administration day (defined as EMT1) and on embryo transfer (ET)day (defined as EMT2) was measured exclusively by transvaginal ultrasound. Inverse probability weighting (IPW) and stratified logistic regressions were conducted to reduce the effects of confounding factors.
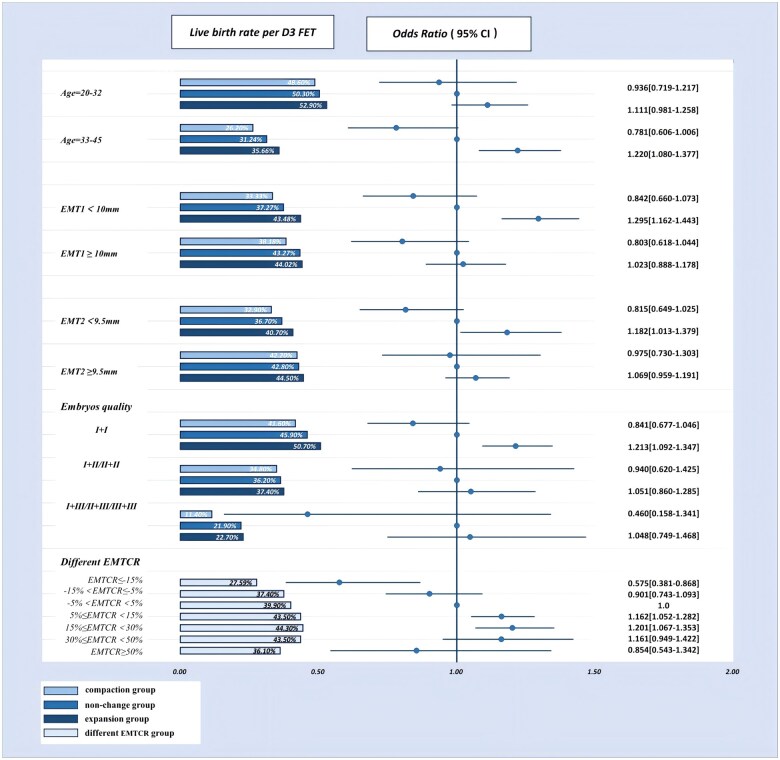
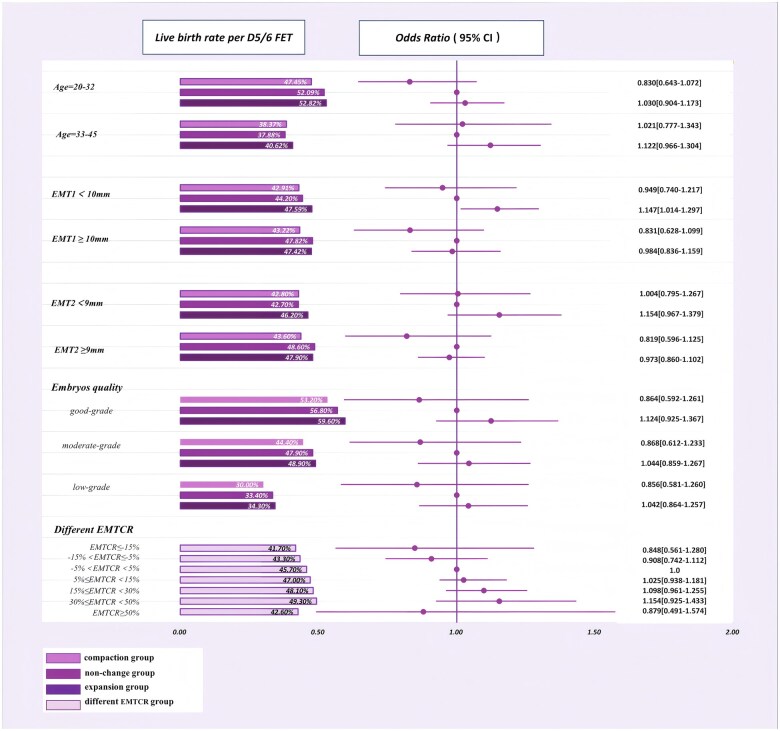
Main results and the role of chance: After IPW adjustment, in D3 FETs, women with compacted endometrium had the lowest HCG-positive rates (P = 0.012), clinical pregnancy rates (P < 0.001), ongoing pregnancy rates (P < 0.001), and live birth rates (LBRs) (P < 0.001) among the three groups. Among HCG-positive cases, the compaction group had the highest ectopic pregnancy rates (3.5% vs 2.6% vs 1.6%; P = 0.015) and the lowest LBRs (65.8% vs 68.3% vs 71.4%; P = 0.018). Univariate logistic regressions found that LBRs were weakly associated with compacted endometrium [odds ratio (OR) 0.831, 95% CI: 0.696-0.993]. Logistic regressions with IPW revealed that the compaction group was not associated with higher odds of pregnancy outcomes, including HCG positive, clinical pregnancy, ongoing pregnancy, ongoing pregnancy, and live births compared to the non-change group. In contrast, the expansion group was associated with higher odds of live birth per ETs (OR 1.166, 95% CI: 1.070-1.271; P = 0.001), and live birth per HCG-positive cases (OR 1.160, 95% CI: 1.028-1.309; P = 0.016). In blastocyst FETs, women with compacted endometrium had the lowest HCG-positive rates (P = 0.001) and clinical pregnancy rates (P = 0.031). Logistic regressions with IPW adjustment found that compaction group was associated with lower odds of HCG positive (OR 0.813, 95% CI: 0.668-0.989, P = 0.039) compared to the non-change group. Additionally, LBRs increased with the rising change ratios of EMT after progesterone administration, but within a certain range (30% in D3 FETs and 50% in blastocyst FETs).
Limitations reasons for caution: This study only included retrospective analyses of untested embryos for FETs.
Wider implications of the findings: Endometrial expansion in D3 FETs exhibited a positive association with improved LBRs, but not in blastocyst FETs. These findings suggest that embryo developmental stage-specific endometrial preparation protocols may enhance assisted reproductive outcomes.
Study funding/competing interests: This study was supported by National Natural Science Foundation of China (82201856), Basic Scientific Research project of Wenzhou Science and Technology Bureau (Y20220006), Wenzhou Key Laboratory of Reproduction and Genetics (2022HZSY0051), and Clinical Technology International Exchange Project of Zhejiang Provincial Medical Institutions. The authors have no conflicts of interest to declare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


