Association of frailty with postoperative outcomes in patients undergoing elective non-malignant abdominal surgeries under general or neuraxial anaesthesia: A prospective observational cohort study.
{"title":"Association of frailty with postoperative outcomes in patients undergoing elective non-malignant abdominal surgeries under general or neuraxial anaesthesia: A prospective observational cohort study.","authors":"Rinu Raju, Pooja Singh, Pranita Mandal, Vaishali Waindeskar, Sunaina Tejpal Karna","doi":"10.4103/ija.ija_903_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Modified frailty index (mFI) is a valuable tool for predicting postoperative complications (POCs). We aimed to determine the association of frailty using mFI and the technique of anaesthesia, with POCs as the primary outcomes in patients undergoing non-malignant abdominal surgeries under general or neuraxial anaesthesia.</p><p><strong>Methods: </strong>After ethical approval, 125 patients of either gender, aged ≥18 years and scheduled to undergo general or neuraxial anaesthesia were enroled. Preoperatively, the mFI score was calculated for all the patients. Patients with mFI ≥0.27 were considered 'significantly frail'. The patients were followed up from the immediate postoperative period to 30 days after surgery, and POCs as per the Clavien-Dindo (CD) classification during their hospital stay were recorded. After discharge, patients were followed up telephonically every 15 days within 30 days to monitor for readmission or mortality.</p><p><strong>Results: </strong>The sensitivity and specificity of the mFI score to predict major POC were 86.11% and 88.76%, respectively, with a high negative predictive value of 94.05%. In mFI scores ≤0.27 and ≥0.27, the odds of POC were 1.74 and 2.33 times higher with general anaesthesia than with neuraxial anaesthesia, respectively. In mFI ≥0.27, the odds of 30-day readmission were 29.04 (95% confidence interval: 6.26, 34.68) with a longer hospital stay (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>Higher mFI scores consistently predict more severe postoperative complications, particularly in CD grades II and IV and intensive care unit. The anaesthesia technique showed no significant association with postoperative complications, except in the higher mFI group.</p>","PeriodicalId":13339,"journal":{"name":"Indian Journal of Anaesthesia","volume":"69 7","pages":"693-699"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12244454/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ija.ija_903_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Modified frailty index (mFI) is a valuable tool for predicting postoperative complications (POCs). We aimed to determine the association of frailty using mFI and the technique of anaesthesia, with POCs as the primary outcomes in patients undergoing non-malignant abdominal surgeries under general or neuraxial anaesthesia.
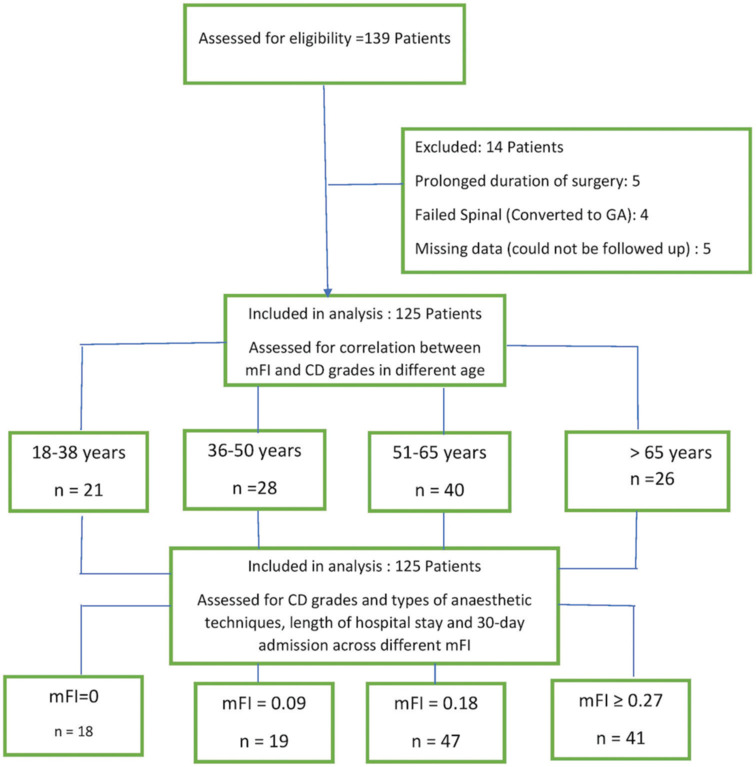
Methods: After ethical approval, 125 patients of either gender, aged ≥18 years and scheduled to undergo general or neuraxial anaesthesia were enroled. Preoperatively, the mFI score was calculated for all the patients. Patients with mFI ≥0.27 were considered 'significantly frail'. The patients were followed up from the immediate postoperative period to 30 days after surgery, and POCs as per the Clavien-Dindo (CD) classification during their hospital stay were recorded. After discharge, patients were followed up telephonically every 15 days within 30 days to monitor for readmission or mortality.
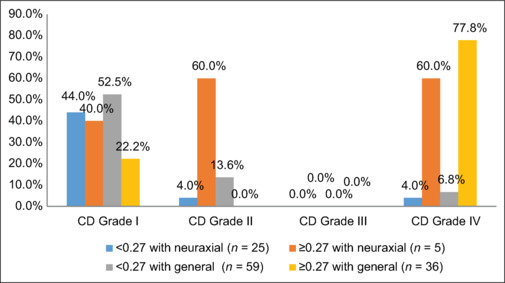
Results: The sensitivity and specificity of the mFI score to predict major POC were 86.11% and 88.76%, respectively, with a high negative predictive value of 94.05%. In mFI scores ≤0.27 and ≥0.27, the odds of POC were 1.74 and 2.33 times higher with general anaesthesia than with neuraxial anaesthesia, respectively. In mFI ≥0.27, the odds of 30-day readmission were 29.04 (95% confidence interval: 6.26, 34.68) with a longer hospital stay (P < 0.001).
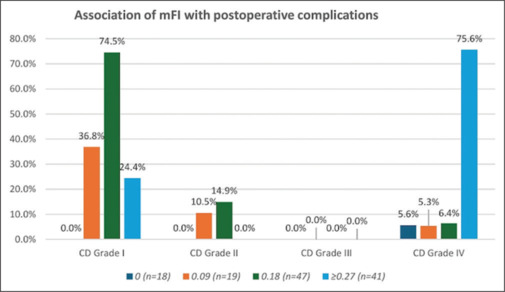
Conclusion: Higher mFI scores consistently predict more severe postoperative complications, particularly in CD grades II and IV and intensive care unit. The anaesthesia technique showed no significant association with postoperative complications, except in the higher mFI group.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


