Cardiac magnetic resonance follow-up of myocardial function in patients with chronic total occlusion of the coronary arteries: a retrospective cohort study.
{"title":"Cardiac magnetic resonance follow-up of myocardial function in patients with chronic total occlusion of the coronary arteries: a retrospective cohort study.","authors":"Jinfan Tian, Libo Liu, Xueyao Yang, Wenxiao Xia, Huijuan Zuo, Haoran Xing, Mingduo Zhang, Min Zhang, Yuan Zhou, Lijun Zhang, Xiantao Song","doi":"10.21037/cdt-24-492","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The impact of percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) on myocardial function remains controversial. This study aims to evaluate changes in myocardial function following CTO-PCI using cardiac magnetic resonance (CMR) imaging and to identify the patient subgroups that derive the greatest benefit from CTO artery recanalization.</p><p><strong>Methods: </strong>We retrospectively screened 652 patients diagnosed with single-vessel CTO through coronary angiography at Beijing Anzhen Hospital between December 2014 and July 2023. Among these, 303 patients underwent baseline CMR imaging, and 115 completed follow-up imaging. A total of 108 patients met the inclusion criteria, with 71 receiving PCI and 37 undergoing optimal medical therapy (OMT). Myocardial viability and cardiac function indices, including left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), and late gadolinium enhancement (LGE) were assessed using CMR. In the subgroup analysis, patients were categorized by LVEF based on clinical consensus (normal: ≥50%; decreased: <50%). Paired t-tests or non-parametric tests were used to compare pre- and post-treatment cardiac function, and Cox regression analysis was performed to identify factors influencing myocardial functional recovery.</p><p><strong>Results: </strong>There were no significant differences between the PCI and OMT groups in baseline characteristics, including age (56.96±10.69 <i>vs.</i> 54.16±11.32 years, P=0.21) and gender distribution [57 (80.3%) <i>vs.</i> 33 (89.2%), P=0.24]. No differences were observed between the PCI and OMT groups in LVEF (61.00%±9.40% <i>vs.</i> 59.68%±9.33%, P=0.50), LVEDV (126.53±31.41 <i>vs.</i> 125.93±29.26 mL, P=0.93), or LVESV [47.09 (35.22, 61.11) <i>vs.</i> 51.41 (36.73, 62.07) mL, P=0.68] at a median follow-up time of 12 months. Additionally, no changes in LVEF, LVEDV, or LVESV were found following PCI (P>0.05). However, in patients with baseline LVEF <50% and segmental LGE ≤50%, LVEF improved post-PCI [46.93% (40.14%, 47.49%) <i>vs.</i> 61.13% (47.48%, 64.54%), P=0.01]. In patients with baseline LVEF <50% and segmental LGE >50%, LVEF was not significantly affected by PCI [43.22% (40.23%, 45.54%) <i>vs.</i> 46.03% (40.75%, 59.06%), P=0.11]. Patients with LVEF ≥50% showed no myocardial function improvements post-PCI, regardless of segmental LGE percentages (P>0.05).</p><p><strong>Conclusions: </strong>Baseline LVEF and myocardial viability assessed via quantitative CMR imaging before CTO-PCI may help select patients who will benefit from the procedure. Although overall LVEF did not improve following CTO-PCI, patients with baseline LVEF <50% and segmental LGE ≤50% benefited more, suggesting the procedure can enhance myocardial function recovery in certain patient groups and confirming the safety and efficacy of CTO-PCI.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"15 3","pages":"610-623"},"PeriodicalIF":2.1000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246994/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-24-492","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The impact of percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) on myocardial function remains controversial. This study aims to evaluate changes in myocardial function following CTO-PCI using cardiac magnetic resonance (CMR) imaging and to identify the patient subgroups that derive the greatest benefit from CTO artery recanalization.
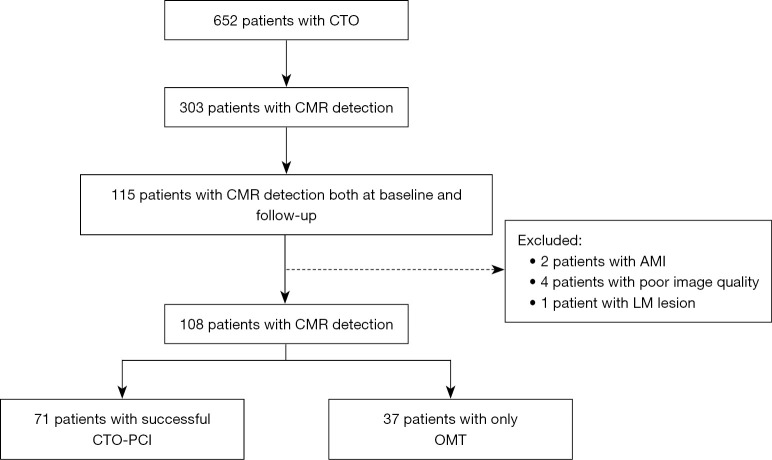
Methods: We retrospectively screened 652 patients diagnosed with single-vessel CTO through coronary angiography at Beijing Anzhen Hospital between December 2014 and July 2023. Among these, 303 patients underwent baseline CMR imaging, and 115 completed follow-up imaging. A total of 108 patients met the inclusion criteria, with 71 receiving PCI and 37 undergoing optimal medical therapy (OMT). Myocardial viability and cardiac function indices, including left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), and late gadolinium enhancement (LGE) were assessed using CMR. In the subgroup analysis, patients were categorized by LVEF based on clinical consensus (normal: ≥50%; decreased: <50%). Paired t-tests or non-parametric tests were used to compare pre- and post-treatment cardiac function, and Cox regression analysis was performed to identify factors influencing myocardial functional recovery.
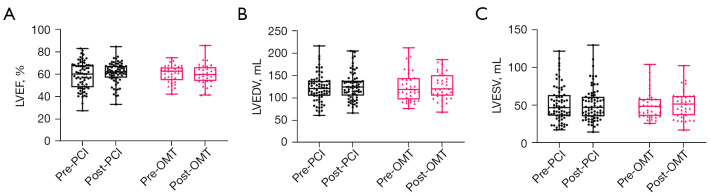
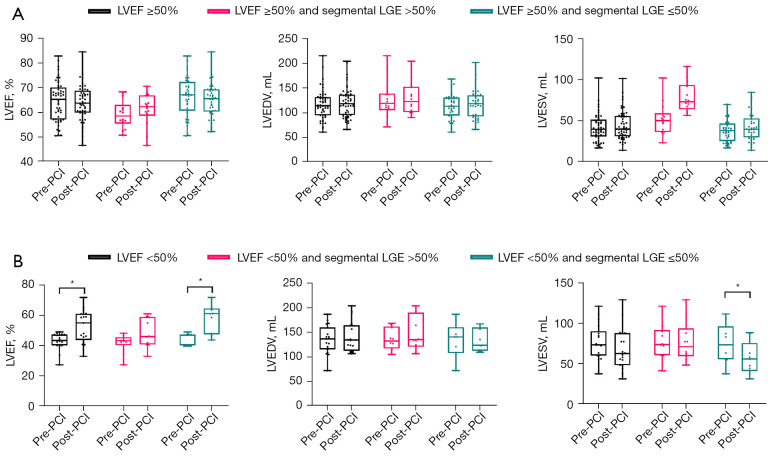
Results: There were no significant differences between the PCI and OMT groups in baseline characteristics, including age (56.96±10.69 vs. 54.16±11.32 years, P=0.21) and gender distribution [57 (80.3%) vs. 33 (89.2%), P=0.24]. No differences were observed between the PCI and OMT groups in LVEF (61.00%±9.40% vs. 59.68%±9.33%, P=0.50), LVEDV (126.53±31.41 vs. 125.93±29.26 mL, P=0.93), or LVESV [47.09 (35.22, 61.11) vs. 51.41 (36.73, 62.07) mL, P=0.68] at a median follow-up time of 12 months. Additionally, no changes in LVEF, LVEDV, or LVESV were found following PCI (P>0.05). However, in patients with baseline LVEF <50% and segmental LGE ≤50%, LVEF improved post-PCI [46.93% (40.14%, 47.49%) vs. 61.13% (47.48%, 64.54%), P=0.01]. In patients with baseline LVEF <50% and segmental LGE >50%, LVEF was not significantly affected by PCI [43.22% (40.23%, 45.54%) vs. 46.03% (40.75%, 59.06%), P=0.11]. Patients with LVEF ≥50% showed no myocardial function improvements post-PCI, regardless of segmental LGE percentages (P>0.05).
Conclusions: Baseline LVEF and myocardial viability assessed via quantitative CMR imaging before CTO-PCI may help select patients who will benefit from the procedure. Although overall LVEF did not improve following CTO-PCI, patients with baseline LVEF <50% and segmental LGE ≤50% benefited more, suggesting the procedure can enhance myocardial function recovery in certain patient groups and confirming the safety and efficacy of CTO-PCI.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


