Weaning from mechanical ventilation in myasthenic crisis according to WEAN safe: most patients experience intermediate or prolonged weaning with no differences between early and late-onset compared to very-late onset myasthenia Gravis.
Clémence Marois, Arthur Combes, Meriem Bouguerra, Alexandra Grinea, Lucas Di Meglio, Thomas Rambaud, Loïc Le Guennec, Francis Bolgert, Benjamin Rohaut, Sophie Demeret, Nicolas Weiss
{"title":"Weaning from mechanical ventilation in myasthenic crisis according to WEAN safe: most patients experience intermediate or prolonged weaning with no differences between early and late-onset compared to very-late onset myasthenia Gravis.","authors":"Clémence Marois, Arthur Combes, Meriem Bouguerra, Alexandra Grinea, Lucas Di Meglio, Thomas Rambaud, Loïc Le Guennec, Francis Bolgert, Benjamin Rohaut, Sophie Demeret, Nicolas Weiss","doi":"10.1186/s13613-025-01515-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Myasthenic crisis often requires prolonged mechanical ventilation and complex weaning, yet data remain scarce. The objective of this study was to describe the weaning characteristics in patients with myasthenic crisis using the WEAN Safe classification. Secondary aims included assessment of long-term outcome and comparison between early- and late-onset (< 65 years) versus very-late-onset MG (≥ 65 years) myasthenia gravis.</p><p><strong>Methods: </strong>This single-center retrospective study included patients admitted for myasthenic crisis to a tertiary neuro-intensive care unit between January 2008 and December 2023. Clinical characteristics, ventilatory support parameters, timing of weaning events, complications, and outcomes were recorded. Weaning was classified according to WEAN Safe definitions: no separation attempt, short wean (successful weaning within 1 day), intermediate wean (2-6 days), prolonged wean (≥ 7 days), or failed wean (persistent invasive ventilation at discharge or death).</p><p><strong>Results: </strong>Among 698 ICU hospitalizations (405 patients) for myasthenia gravis, 131 (120 patients) received invasive mechanical ventilation. Fifty hospitalizations (39 patients) were excluded due to non-MC-related intubation, insufficient weaning data or patients with multiple ICU admissions. The final analysis included 81 patients (median age 70 years [54-81]; 43% female; 64% with very-late-onset myasthenia gravis (≥ 65 years). The median duration of mechanical ventilation was 20 days [11-38], and the median time from the first separation attempt to successful weaning was 7 days [3-19]. According to the WEAN Safe classification, 3% had a short wean, 40% intermediate, 55% prolonged, and 3% failed weaning. Four patients (5%) required reintubation within 48 h. Ventilator-associated pneumonia occurred in 15% of patients before the first separation attempt. In multivariate analysis, the presence of thymoma (OR 3.02, 95% CI 1.01-9.07) and absence of MG-specific immunosuppressive treatment at ICU admission (OR 3.70, 95% CI 1.22-11.23) were independently associated with prolonged weaning. Intensive care unit mortality was 7%, and 12-month mortality was 19%. The median myasthenic muscle score at 1 year was 94/100 [80-100]. No significant differences in weaning parameters nor outcome were found between early- and late-onset versus very-late-onset MG, despite more comorbidities in the very-late-onset group.</p><p><strong>Conclusions: </strong>In this retrospective study from a single expert center, most patients with myasthenic crisis underwent intermediate or prolonged weaning, but extubation failure rate was very low. Thymoma and lack of MG-specific immunosuppressive treatment at ICU admission are associated with prolonged weaning, while age alone is not. Despite initial challenges, long-term outcomes are generally favorable, highlighting the reversibility of myasthenic crisis with expert care.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"95"},"PeriodicalIF":5.5000,"publicationDate":"2025-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12259497/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01515-2","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Myasthenic crisis often requires prolonged mechanical ventilation and complex weaning, yet data remain scarce. The objective of this study was to describe the weaning characteristics in patients with myasthenic crisis using the WEAN Safe classification. Secondary aims included assessment of long-term outcome and comparison between early- and late-onset (< 65 years) versus very-late-onset MG (≥ 65 years) myasthenia gravis.
Methods: This single-center retrospective study included patients admitted for myasthenic crisis to a tertiary neuro-intensive care unit between January 2008 and December 2023. Clinical characteristics, ventilatory support parameters, timing of weaning events, complications, and outcomes were recorded. Weaning was classified according to WEAN Safe definitions: no separation attempt, short wean (successful weaning within 1 day), intermediate wean (2-6 days), prolonged wean (≥ 7 days), or failed wean (persistent invasive ventilation at discharge or death).
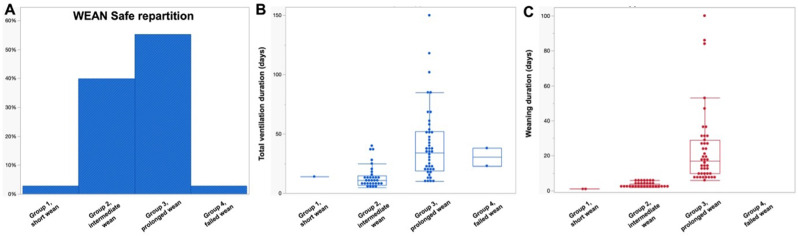
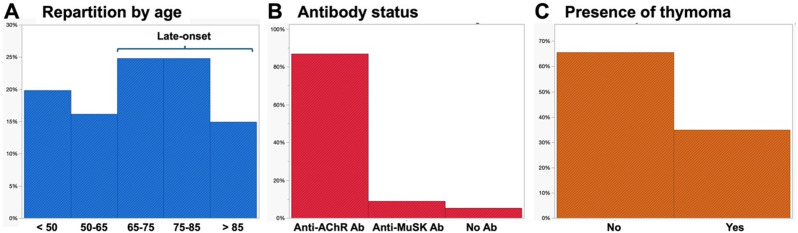
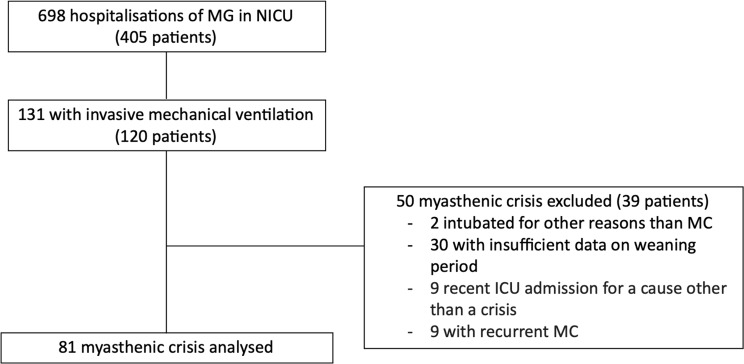
Results: Among 698 ICU hospitalizations (405 patients) for myasthenia gravis, 131 (120 patients) received invasive mechanical ventilation. Fifty hospitalizations (39 patients) were excluded due to non-MC-related intubation, insufficient weaning data or patients with multiple ICU admissions. The final analysis included 81 patients (median age 70 years [54-81]; 43% female; 64% with very-late-onset myasthenia gravis (≥ 65 years). The median duration of mechanical ventilation was 20 days [11-38], and the median time from the first separation attempt to successful weaning was 7 days [3-19]. According to the WEAN Safe classification, 3% had a short wean, 40% intermediate, 55% prolonged, and 3% failed weaning. Four patients (5%) required reintubation within 48 h. Ventilator-associated pneumonia occurred in 15% of patients before the first separation attempt. In multivariate analysis, the presence of thymoma (OR 3.02, 95% CI 1.01-9.07) and absence of MG-specific immunosuppressive treatment at ICU admission (OR 3.70, 95% CI 1.22-11.23) were independently associated with prolonged weaning. Intensive care unit mortality was 7%, and 12-month mortality was 19%. The median myasthenic muscle score at 1 year was 94/100 [80-100]. No significant differences in weaning parameters nor outcome were found between early- and late-onset versus very-late-onset MG, despite more comorbidities in the very-late-onset group.
Conclusions: In this retrospective study from a single expert center, most patients with myasthenic crisis underwent intermediate or prolonged weaning, but extubation failure rate was very low. Thymoma and lack of MG-specific immunosuppressive treatment at ICU admission are associated with prolonged weaning, while age alone is not. Despite initial challenges, long-term outcomes are generally favorable, highlighting the reversibility of myasthenic crisis with expert care.
背景:肌无力危机通常需要长时间的机械通气和复杂的脱机,但数据仍然很少。本研究的目的是使用断奶安全分类来描述肌无力危象患者的断奶特征。次要目的包括评估长期结果并比较早发和晚发(方法:这项单中心回顾性研究纳入了2008年1月至2023年12月期间因肌无力危重症入住三级神经重症监护病房的患者。记录临床特征、呼吸支持参数、脱机时间、并发症和结果。根据断奶安全定义将断奶分为:无分离尝试、短期断奶(1天内成功断奶)、中期断奶(2-6天)、延长断奶(≥7天)或失败断奶(出院或死亡时持续有创通气)。结果:698例(405例)重症肌无力ICU住院患者中,有创机械通气131例(120例)。50例住院患者(39例)因非mc相关插管、不充分的脱机数据或多次入住ICU的患者被排除。最终分析纳入81例患者(中位年龄70岁[54-81];43%的女性;64%为极晚发性重症肌无力(≥65岁)。机械通气的中位持续时间为20天[11-38],从首次分离尝试到成功脱机的中位时间为7天[3-19]。根据断奶安全分类,3%为短期断奶,40%为中期断奶,55%为延长断奶,3%为失败断奶。4名患者(5%)在48小时内需要重新插管。15%的患者在第一次分离尝试前发生呼吸机相关性肺炎。在多因素分析中,在ICU入院时胸腺瘤的存在(OR 3.02, 95% CI 1.01-9.07)和未接受mg特异性免疫抑制治疗(OR 3.70, 95% CI 1.22-11.23)与延长脱机时间独立相关。重症监护病房死亡率为7%,12个月死亡率为19%。1年时肌无力评分中位数为94/100[80-100]。早发性、晚发性MG与极晚发性MG在断奶参数和结局上没有显著差异,尽管极晚发性MG有更多合并症。结论:本回顾性研究来自单一专家中心,大多数肌无力危象患者均行中期或长时间脱机,但拔管失败率很低。在ICU入院时胸腺瘤和缺乏mg特异性免疫抑制治疗与脱机时间延长有关,而年龄本身与脱机时间延长无关。尽管最初的挑战,长期的结果通常是有利的,强调重症肌无力危机的可逆性与专家护理。
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


