Ida M. Heerfordt, Espen Jimenez-Solem, Magnus Middelboe, Rasmus Huan Olsen, Henrik Horwitz
{"title":"Risk of Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis Associated With Mebendazole Use","authors":"Ida M. Heerfordt, Espen Jimenez-Solem, Magnus Middelboe, Rasmus Huan Olsen, Henrik Horwitz","doi":"10.1111/bcpt.70086","DOIUrl":null,"url":null,"abstract":"<p>Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but potentially fatal conditions, most often caused by adverse reactions to medication [<span>1</span>]. They are characterized by widespread skin necrosis and detachment of the epidermis [<span>1</span>]. The conditions are considered part of a disease spectrum, differentiated primarily by the extent of skin involvement [<span>1</span>]. It is accepted that the triggering medication is generally used within 3 months before symptom onset [<span>1</span>].</p><p>Mebendazole, a commonly used anthelmintic in both children and adults, has rarely been associated with SJS and TEN, primarily through isolated case series [<span>2</span>]. Mebendazole acts by binding to a subunit of helminthic tubulin, inhibiting microtubule formation and thereby disrupting essential cellular processes [<span>3</span>]. While patient labels for mebendazole cite occurrences of SJS and TEN as rare, listed as occurring in between 1 in 10 000 and 1 in 1000 treatments, the actual risk has not been quantified in large-scale, population-based studies [<span>2, 4-6</span>].</p><p>This study aimed to quantify the risk of developing SJS and TEN associated with mebendazole usage, to alleviate fears and improve the clinical basis for rational decision-making in prescribing.</p><p>This study employed a nationwide, population-based design using the Danish National Health Registries [<span>7</span>]. All Danish residents are systematically registered in the Danish Civil Registration System with a unique personal identification number, enabling precise linkage across health registries [<span>7</span>].</p><p>First, we established a cohort consisting of the entire Danish population from 1994 to 2025. Using the Danish National Prescription Register [<span>7</span>], we identified all individuals who redeemed at least one prescription for mebendazole (Anatomical Therapeutic Chemical (ATC) code P02CA01). The Danish National Patient Register was used to identify all cases of first-time diagnosis of erythema multiforme bullosum/SJS (International Classification of Diseases, 10th Revision (ICD-10) code L51.1) or TEN (ICD-10 code L51.2) during the same period. Patients assigned both diagnoses were included on equal terms with those assigned only one diagnosis. Based on this cohort, we calculated the absolute frequency of SJS/TEN following mebendazole use.</p><p>Second, we conducted a nested case–control study within the same cohort. All individuals with a first-time diagnosis of SJS or TEN were identified as cases. For each case, 100 controls were selected using risk set sampling, matched on age, sex and index date, based on data from the Danish Civil Registration System. Participants were required to have been residents in Denmark for at least 1 year prior to the index date. Mebendazole prescription retrieval was assessed for both cases and controls during two exposure windows: within 3 months and within 12 months before the index date. All prescription data were obtained from the Danish National Prescription Register identified using ATC code P02CA01.</p><p>Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). For the cohort study, we calculated the absolute frequency of SJS/TEN following mebendazole use by descriptive analysis. For the nested case–control study, we compared the proportion of mebendazole prescriptions in cases and controls and estimated the potential association between mebendazole use and the occurrence of SJS/TEN. We calculated odds ratios and 95% CI from a conditional logistic regression model. A schematic overview of the study designs is presented in Figure 1.</p><p>The study was conducted in accordance with the <i>Basic & Clinical Pharmacology & Toxicology</i> policy for data studies [<span>8</span>]. The Danish Data Protection Agency (p-2024-15764) and the Danish National Board of Health (FSEID-00007077) approved this research. Danish regulations prevented the reporting of specific figures between 1 and 4 and the calculation of exact <i>p</i>-values or odds ratios to protect data confidentiality.</p><p>Between 1994 and 2025, the Danish population consisted of 9.33 million individuals, contributing 171 million person-years at risk. In this timeframe, 2.66 million prescriptions for mebendazole were redeemed by approximately 1.18 million individuals. Between 1 and 4 individuals developed SJS/TEN within 3 months after redeeming a mebendazole prescription. Thus, the observed frequency of SJS/TEN occurring within 3 months after mebendazole treatment was fewer than 1 in 450 000 prescriptions.</p><p>We identified a total of 1204 incident cases of SJS or TEN in Denmark. Of these, 1185 individuals had been Danish residents for at least 1 year prior to diagnosis and were included in the study. The average age at diagnosis was 43 years, and 46.6% of the patients were females. The controls were matched by age and sex; see Table 1.</p><p>In the 3-month window prior to diagnosis, between 1 and 4 of the cases had redeemed a prescription for mebendazole, corresponding to 0.08%–0.34% of the cases. Among the 118 500 matched controls, 275 had used mebendazole in the same period (0.23%). According to Danish data protection regulations, the exact number of exposed cases cannot be disclosed, and the resulting odds ratio cannot be calculated for this period. However, given the low number of exposed cases, any potential association is statistically insignificant.</p><p>Extending the exposure period to 12 months prior to diagnosis, 14 of the cases (1.18%) and 1295 of the controls (1.09%) had redeemed at least one mebendazole prescription. This yielded an odds ratio of 1.08 (95% CI: 0.63–1.86; <i>p</i> = 0.76), indicating no significant association between mebendazole use and the development of SJS or TEN.</p><p>This nationwide, population-based study found no significant association between mebendazole use and the development of SJS or TEN. Among more than 2.6 million redeemed prescriptions over a 31-year period, fewer than five cases of SJS/TEN were observed within 3 months after mebendazole use, corresponding to a frequency of less than 1 in 450 000 treatments. This is markedly lower than the incidence suggested in product labeling, which typically estimates the risk between 1 in 10 000 and 1 in 1000 treatments [<span>4-6</span>].</p><p>A risk as high as 1 per 1000 treated individuals for developing SJS/TEN would be particularly problematic for the indication of pinworms, as it is generally recommended to treat the entire household, including asymptomatic individuals [<span>9</span>].</p><p>While previous case reports have raised concern, especially in the context of comedication or outbreaks, our findings suggest that such events are exceedingly rare and may not reflect a causal relationship in routine clinical settings [<span>2</span>].</p><p>According to the European Medicines Agency guideline on summaries of product characteristics, frequencies of adverse reactions should be based on data from clinical trials, postauthorization safety studies and spontaneous reporting systems, where a causal relationship is at least reasonably possible [<span>10</span>]. However, it is increasingly recognized that estimates from these sources may not accurately reflect the true population risk [<span>11</span>]. Especially in cases where side effects are discovered postmarketing, it can be difficult to estimate the risk. Here, the manufacturer may choose to estimate the risk based on the ‘rule of three’, as the 95% confidence interval around 0 can be at most 3. If no cases of the new side effect were observed during the clinical trial, it cannot be excluded that there could have been three cases. The risk is thus estimated as 3 divided by the number of patients who participated in the clinical studies. Such a risk estimate will, by nature, be an absolute worst case scenario [<span>10</span>].</p><p>There are some limitations inherent to this study. First, mebendazole exposure not captured in the Danish National Prescription Register, such as purchases abroad or intrahousehold sharing of medication, could result in underestimation of true exposure. While this misclassification is unlikely to affect the calculated absolute risk observed in the cohort study, it may lead to exposure misclassification among controls in the case–control study. Second, misclassification of diagnoses is possible. The diagnosis of TEN has been validated in Danish health registries, whereas the SJS code is grouped together with erythema multiforme bullosum, which is less severe than SJS [<span>12</span>]. Consequently, the incidence of SJS may be overestimated. However, the fact that we could not report the number of cases of SJS/TEN after exposure to mebendazole according to Danish data protection legislation confirms that the risk of developing this condition is extremely rare, and it is doubtful whether there is any association at all. Finally, it should be mentioned that the study was conducted in a Danish population, which is relatively ethnically homogeneous, and whether the results translate into other populations will require further investigations. Due to the limited sample size, it was also not possible to investigate the impact of comedication, which will require future studies with larger populations.</p><p>In conclusion, our results support the continued safe use of mebendazole and provide reassuring evidence for clinicians and patients.</p><p>Ida M. Heerfordt, Espen Jimenez-Solem, Rasmus Huan Olsen and Henrik Horwitz contributed to the study conception and design. Ida M. Heerfordt, Magnus Middelboe, Rasmus Huan Olsen and Henrik Horwitz performed data collection and analysis. Ida M. Heerfordt wrote the first draft of the manuscript, and all authors reviewed and commented on subsequent versions. All authors read and approved the final manuscript.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":8733,"journal":{"name":"Basic & Clinical Pharmacology & Toxicology","volume":"137 2","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bcpt.70086","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Basic & Clinical Pharmacology & Toxicology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bcpt.70086","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but potentially fatal conditions, most often caused by adverse reactions to medication [1]. They are characterized by widespread skin necrosis and detachment of the epidermis [1]. The conditions are considered part of a disease spectrum, differentiated primarily by the extent of skin involvement [1]. It is accepted that the triggering medication is generally used within 3 months before symptom onset [1].
Mebendazole, a commonly used anthelmintic in both children and adults, has rarely been associated with SJS and TEN, primarily through isolated case series [2]. Mebendazole acts by binding to a subunit of helminthic tubulin, inhibiting microtubule formation and thereby disrupting essential cellular processes [3]. While patient labels for mebendazole cite occurrences of SJS and TEN as rare, listed as occurring in between 1 in 10 000 and 1 in 1000 treatments, the actual risk has not been quantified in large-scale, population-based studies [2, 4-6].
This study aimed to quantify the risk of developing SJS and TEN associated with mebendazole usage, to alleviate fears and improve the clinical basis for rational decision-making in prescribing.
This study employed a nationwide, population-based design using the Danish National Health Registries [7]. All Danish residents are systematically registered in the Danish Civil Registration System with a unique personal identification number, enabling precise linkage across health registries [7].
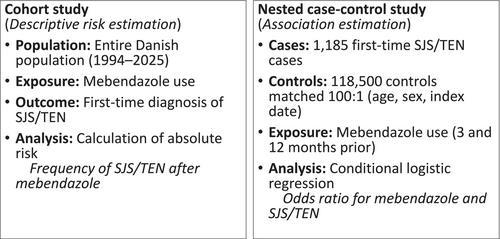
First, we established a cohort consisting of the entire Danish population from 1994 to 2025. Using the Danish National Prescription Register [7], we identified all individuals who redeemed at least one prescription for mebendazole (Anatomical Therapeutic Chemical (ATC) code P02CA01). The Danish National Patient Register was used to identify all cases of first-time diagnosis of erythema multiforme bullosum/SJS (International Classification of Diseases, 10th Revision (ICD-10) code L51.1) or TEN (ICD-10 code L51.2) during the same period. Patients assigned both diagnoses were included on equal terms with those assigned only one diagnosis. Based on this cohort, we calculated the absolute frequency of SJS/TEN following mebendazole use.
Second, we conducted a nested case–control study within the same cohort. All individuals with a first-time diagnosis of SJS or TEN were identified as cases. For each case, 100 controls were selected using risk set sampling, matched on age, sex and index date, based on data from the Danish Civil Registration System. Participants were required to have been residents in Denmark for at least 1 year prior to the index date. Mebendazole prescription retrieval was assessed for both cases and controls during two exposure windows: within 3 months and within 12 months before the index date. All prescription data were obtained from the Danish National Prescription Register identified using ATC code P02CA01.
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). For the cohort study, we calculated the absolute frequency of SJS/TEN following mebendazole use by descriptive analysis. For the nested case–control study, we compared the proportion of mebendazole prescriptions in cases and controls and estimated the potential association between mebendazole use and the occurrence of SJS/TEN. We calculated odds ratios and 95% CI from a conditional logistic regression model. A schematic overview of the study designs is presented in Figure 1.
The study was conducted in accordance with the Basic & Clinical Pharmacology & Toxicology policy for data studies [8]. The Danish Data Protection Agency (p-2024-15764) and the Danish National Board of Health (FSEID-00007077) approved this research. Danish regulations prevented the reporting of specific figures between 1 and 4 and the calculation of exact p-values or odds ratios to protect data confidentiality.
Between 1994 and 2025, the Danish population consisted of 9.33 million individuals, contributing 171 million person-years at risk. In this timeframe, 2.66 million prescriptions for mebendazole were redeemed by approximately 1.18 million individuals. Between 1 and 4 individuals developed SJS/TEN within 3 months after redeeming a mebendazole prescription. Thus, the observed frequency of SJS/TEN occurring within 3 months after mebendazole treatment was fewer than 1 in 450 000 prescriptions.
We identified a total of 1204 incident cases of SJS or TEN in Denmark. Of these, 1185 individuals had been Danish residents for at least 1 year prior to diagnosis and were included in the study. The average age at diagnosis was 43 years, and 46.6% of the patients were females. The controls were matched by age and sex; see Table 1.
In the 3-month window prior to diagnosis, between 1 and 4 of the cases had redeemed a prescription for mebendazole, corresponding to 0.08%–0.34% of the cases. Among the 118 500 matched controls, 275 had used mebendazole in the same period (0.23%). According to Danish data protection regulations, the exact number of exposed cases cannot be disclosed, and the resulting odds ratio cannot be calculated for this period. However, given the low number of exposed cases, any potential association is statistically insignificant.
Extending the exposure period to 12 months prior to diagnosis, 14 of the cases (1.18%) and 1295 of the controls (1.09%) had redeemed at least one mebendazole prescription. This yielded an odds ratio of 1.08 (95% CI: 0.63–1.86; p = 0.76), indicating no significant association between mebendazole use and the development of SJS or TEN.
This nationwide, population-based study found no significant association between mebendazole use and the development of SJS or TEN. Among more than 2.6 million redeemed prescriptions over a 31-year period, fewer than five cases of SJS/TEN were observed within 3 months after mebendazole use, corresponding to a frequency of less than 1 in 450 000 treatments. This is markedly lower than the incidence suggested in product labeling, which typically estimates the risk between 1 in 10 000 and 1 in 1000 treatments [4-6].
A risk as high as 1 per 1000 treated individuals for developing SJS/TEN would be particularly problematic for the indication of pinworms, as it is generally recommended to treat the entire household, including asymptomatic individuals [9].
While previous case reports have raised concern, especially in the context of comedication or outbreaks, our findings suggest that such events are exceedingly rare and may not reflect a causal relationship in routine clinical settings [2].
According to the European Medicines Agency guideline on summaries of product characteristics, frequencies of adverse reactions should be based on data from clinical trials, postauthorization safety studies and spontaneous reporting systems, where a causal relationship is at least reasonably possible [10]. However, it is increasingly recognized that estimates from these sources may not accurately reflect the true population risk [11]. Especially in cases where side effects are discovered postmarketing, it can be difficult to estimate the risk. Here, the manufacturer may choose to estimate the risk based on the ‘rule of three’, as the 95% confidence interval around 0 can be at most 3. If no cases of the new side effect were observed during the clinical trial, it cannot be excluded that there could have been three cases. The risk is thus estimated as 3 divided by the number of patients who participated in the clinical studies. Such a risk estimate will, by nature, be an absolute worst case scenario [10].
There are some limitations inherent to this study. First, mebendazole exposure not captured in the Danish National Prescription Register, such as purchases abroad or intrahousehold sharing of medication, could result in underestimation of true exposure. While this misclassification is unlikely to affect the calculated absolute risk observed in the cohort study, it may lead to exposure misclassification among controls in the case–control study. Second, misclassification of diagnoses is possible. The diagnosis of TEN has been validated in Danish health registries, whereas the SJS code is grouped together with erythema multiforme bullosum, which is less severe than SJS [12]. Consequently, the incidence of SJS may be overestimated. However, the fact that we could not report the number of cases of SJS/TEN after exposure to mebendazole according to Danish data protection legislation confirms that the risk of developing this condition is extremely rare, and it is doubtful whether there is any association at all. Finally, it should be mentioned that the study was conducted in a Danish population, which is relatively ethnically homogeneous, and whether the results translate into other populations will require further investigations. Due to the limited sample size, it was also not possible to investigate the impact of comedication, which will require future studies with larger populations.
In conclusion, our results support the continued safe use of mebendazole and provide reassuring evidence for clinicians and patients.
Ida M. Heerfordt, Espen Jimenez-Solem, Rasmus Huan Olsen and Henrik Horwitz contributed to the study conception and design. Ida M. Heerfordt, Magnus Middelboe, Rasmus Huan Olsen and Henrik Horwitz performed data collection and analysis. Ida M. Heerfordt wrote the first draft of the manuscript, and all authors reviewed and commented on subsequent versions. All authors read and approved the final manuscript.
期刊介绍:
Basic & Clinical Pharmacology and Toxicology is an independent journal, publishing original scientific research in all fields of toxicology, basic and clinical pharmacology. This includes experimental animal pharmacology and toxicology and molecular (-genetic), biochemical and cellular pharmacology and toxicology. It also includes all aspects of clinical pharmacology: pharmacokinetics, pharmacodynamics, therapeutic drug monitoring, drug/drug interactions, pharmacogenetics/-genomics, pharmacoepidemiology, pharmacovigilance, pharmacoeconomics, randomized controlled clinical trials and rational pharmacotherapy. For all compounds used in the studies, the chemical constitution and composition should be known, also for natural compounds.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


