Surgical and diagnostic management challenges of giant Wilms tumor with intracardial and IVC thrombus extension in a 3-year-old: A rare case from a resource-limited facility involving global and local pediatric surgical teams.
Mathayo Shadrack, Bernard Philip Magoda, Novath Ngowi, Victor Ngotta, Zaituni Bokhary, Martin Thomas Corbally
{"title":"Surgical and diagnostic management challenges of giant Wilms tumor with intracardial and IVC thrombus extension in a 3-year-old: A rare case from a resource-limited facility involving global and local pediatric surgical teams.","authors":"Mathayo Shadrack, Bernard Philip Magoda, Novath Ngowi, Victor Ngotta, Zaituni Bokhary, Martin Thomas Corbally","doi":"10.1016/j.ijscr.2025.111611","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Wilms tumor (nephroblastoma) is the most common renal malignancy in pediatric population, typically diagnosed before the age of 5. Vascular extension into the inferior vena cava (IVC) is seen in approximately 4-10 % of cases, but intracardiac extension, particularly into the right atrium, is exceedingly rare. Managing such advanced tumors in resource-limited settings presents major diagnostic and surgical challenges.</p><p><strong>Case presentation: </strong>Herein a rare case of a 3-year-old boy presenting with a giant Wilms tumor exhibiting extensive intravascular spread. Preoperative CT scans of the chest and abdomen revealed significant invasion into the IVC with thrombus extending into the right atrium. The patient underwent neoadjuvant chemotherapy, which led to marked tumor and thrombus reduction. Intraoperatively, the tumor was found adherent to the colon and left common iliac artery but was dissected without arterial injury. A massive intravascular thrombus was identified, forming a wandering thrombus, with evidence of collateral venous drainage indicating longstanding IVC obstruction. Cavotomy was performed, and the IVC was completely transected without hemodynamic compromise due to collateralization. The surgery was uneventful, and the patient recovered in the Pediatric Intensive Care Unit (PICU).</p><p><strong>Discussion: </strong>This case highlights the complexity of managing extensive Wilms tumor thrombus with intracardiac involvement in a low-resource environment. It underscores the role of neoadjuvant chemotherapy and surgical planning in achieving curative resection.</p><p><strong>Conclusion: </strong>Multidisciplinary coordination, preoperative chemotherapy, and understanding of collateral circulation allowed successful management of this rare and complex Wilms tumor case in a resource-constrained setting.</p>","PeriodicalId":48113,"journal":{"name":"International Journal of Surgery Case Reports","volume":"133 ","pages":"111611"},"PeriodicalIF":0.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12275882/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Surgery Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.ijscr.2025.111611","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/5 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Wilms tumor (nephroblastoma) is the most common renal malignancy in pediatric population, typically diagnosed before the age of 5. Vascular extension into the inferior vena cava (IVC) is seen in approximately 4-10 % of cases, but intracardiac extension, particularly into the right atrium, is exceedingly rare. Managing such advanced tumors in resource-limited settings presents major diagnostic and surgical challenges.
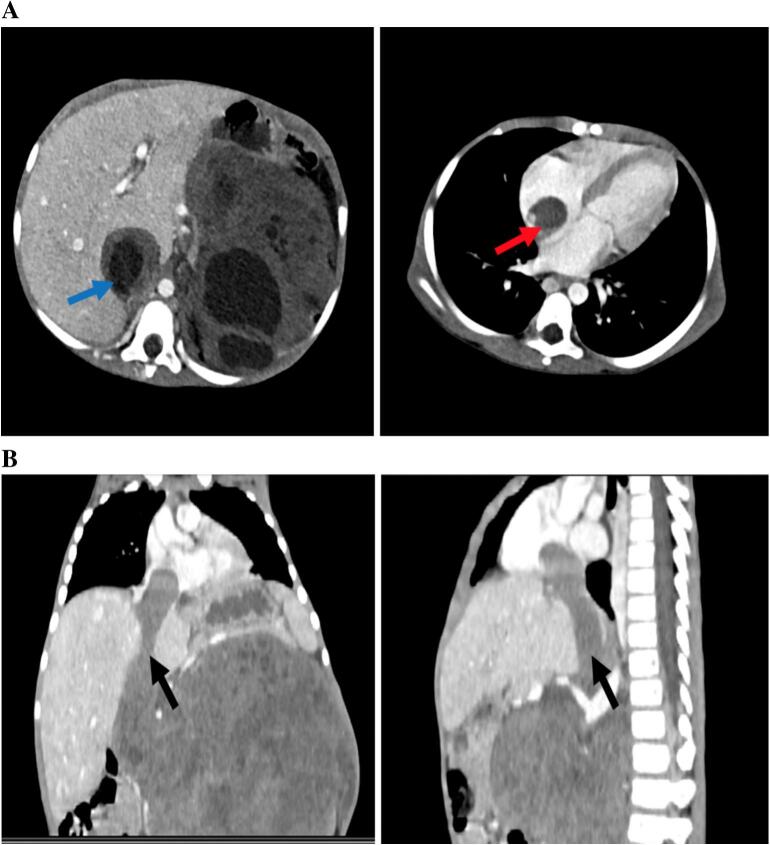
Case presentation: Herein a rare case of a 3-year-old boy presenting with a giant Wilms tumor exhibiting extensive intravascular spread. Preoperative CT scans of the chest and abdomen revealed significant invasion into the IVC with thrombus extending into the right atrium. The patient underwent neoadjuvant chemotherapy, which led to marked tumor and thrombus reduction. Intraoperatively, the tumor was found adherent to the colon and left common iliac artery but was dissected without arterial injury. A massive intravascular thrombus was identified, forming a wandering thrombus, with evidence of collateral venous drainage indicating longstanding IVC obstruction. Cavotomy was performed, and the IVC was completely transected without hemodynamic compromise due to collateralization. The surgery was uneventful, and the patient recovered in the Pediatric Intensive Care Unit (PICU).
Discussion: This case highlights the complexity of managing extensive Wilms tumor thrombus with intracardiac involvement in a low-resource environment. It underscores the role of neoadjuvant chemotherapy and surgical planning in achieving curative resection.
Conclusion: Multidisciplinary coordination, preoperative chemotherapy, and understanding of collateral circulation allowed successful management of this rare and complex Wilms tumor case in a resource-constrained setting.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


