Lisa M Rickey, Katharine Nagle, Julia Perkins, Caroline Kohler, Benjamin Ethier, Kristen Fontaine, Susan Matherson, Anne M Stack, Maireade E McSweeney
{"title":"Standardization Improves Discharge Care Coordination for Children with Nasogastric Tubes.","authors":"Lisa M Rickey, Katharine Nagle, Julia Perkins, Caroline Kohler, Benjamin Ethier, Kristen Fontaine, Susan Matherson, Anne M Stack, Maireade E McSweeney","doi":"10.1097/pq9.0000000000000823","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Discharging patients with new nasogastric tubes (NGTs) for enteral nutrition at home is complex and requires intricate care coordination and education from a multidisciplinary team. We designed a quality improvement (QI) initiative to improve efficiency and decrease variation in care coordination for patients discharged with a new NGT. Our objective was to reduce mean modified hospital length of stay (mLOS) by 10% from baseline within 6 months and sustain improvement for 12 months.</p><p><strong>Methods: </strong>Applying the Model for Improvement, we used plan-do-study-act cycles to improve NGT discharge care coordination using a multidisciplinary team. Primary interventions rooted in Lean methodology included creating a standardized discharge algorithm, utilizing nurse practitioners as care coordination champions, routine consultation of an enteral tube service (ETS), and implementing a formula substitution guide. The primary outcome measure was mean mLOS. The process measure was the time from NGT placement to ETS consult. Balancing measures were ETS consult volume and 30-day healthcare reutilization. Statistical process control charts measured the impact of interventions.</p><p><strong>Results: </strong>Baseline mLOS decreased from 8.2 to 7.4 days with a sustained reduction in process variability over time. Time from NGT placement to ETS consult decreased from 4.1 to 3.0 days. There were no changes in 30-day healthcare reutilization or ETS consult volume over time.</p><p><strong>Conclusions: </strong>A multidisciplinary quality improvement initiative effectively improved complex NGT transitional care planning and was sustained over time.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 4","pages":"e823"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245309/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000823","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
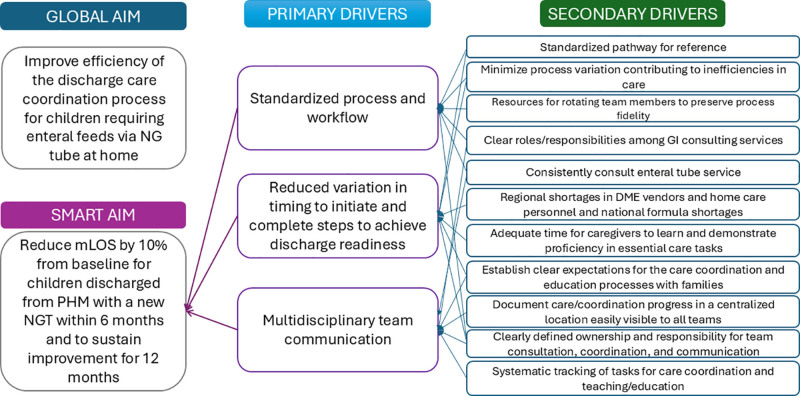
Introduction: Discharging patients with new nasogastric tubes (NGTs) for enteral nutrition at home is complex and requires intricate care coordination and education from a multidisciplinary team. We designed a quality improvement (QI) initiative to improve efficiency and decrease variation in care coordination for patients discharged with a new NGT. Our objective was to reduce mean modified hospital length of stay (mLOS) by 10% from baseline within 6 months and sustain improvement for 12 months.
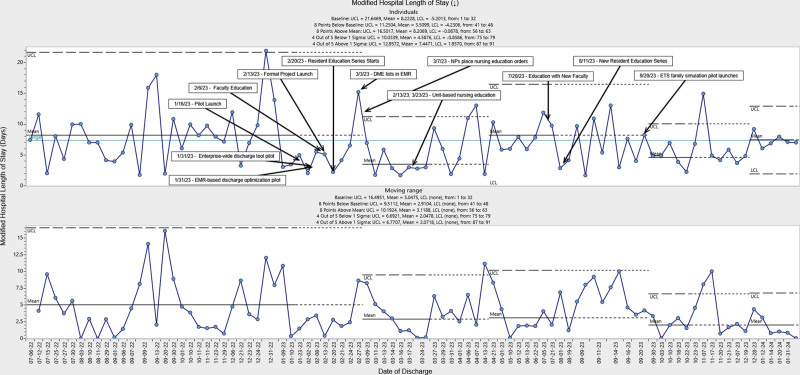
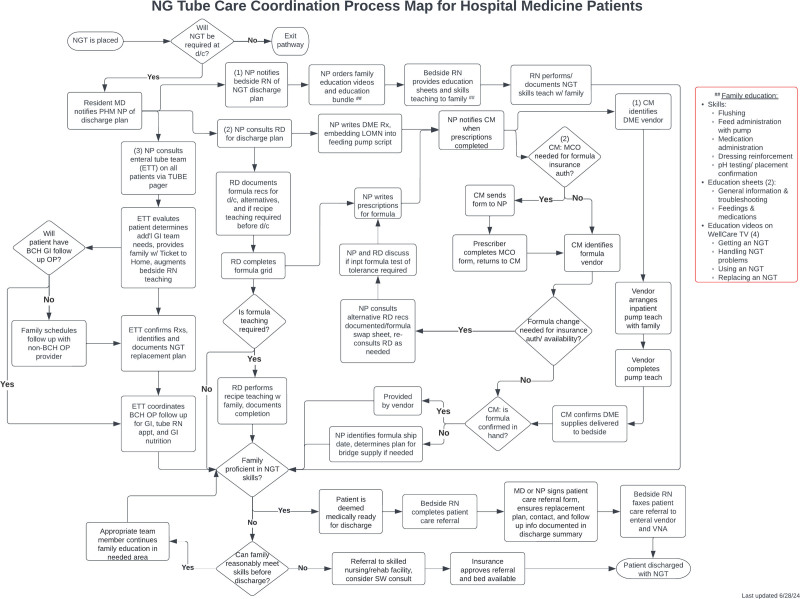
Methods: Applying the Model for Improvement, we used plan-do-study-act cycles to improve NGT discharge care coordination using a multidisciplinary team. Primary interventions rooted in Lean methodology included creating a standardized discharge algorithm, utilizing nurse practitioners as care coordination champions, routine consultation of an enteral tube service (ETS), and implementing a formula substitution guide. The primary outcome measure was mean mLOS. The process measure was the time from NGT placement to ETS consult. Balancing measures were ETS consult volume and 30-day healthcare reutilization. Statistical process control charts measured the impact of interventions.
Results: Baseline mLOS decreased from 8.2 to 7.4 days with a sustained reduction in process variability over time. Time from NGT placement to ETS consult decreased from 4.1 to 3.0 days. There were no changes in 30-day healthcare reutilization or ETS consult volume over time.
Conclusions: A multidisciplinary quality improvement initiative effectively improved complex NGT transitional care planning and was sustained over time.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


