Efficacy of indocyanine green fluorescence-based near-infrared angiography in assessing intraoperative wound perfusion for bone and soft-tissue surgery.
Han Wang, Xiaodong Tang, Tao Ji, Dasen Li, Huayi Qu, Zhiye Du, Wei Guo
{"title":"Efficacy of indocyanine green fluorescence-based near-infrared angiography in assessing intraoperative wound perfusion for bone and soft-tissue surgery.","authors":"Han Wang, Xiaodong Tang, Tao Ji, Dasen Li, Huayi Qu, Zhiye Du, Wei Guo","doi":"10.1302/2633-1462.67.BJO-2024-0248.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Wound complication is common in bone and soft-tissue tumour surgery. Proper wound healing requires robust blood perfusion. However, intraoperative assessment of perfusion is difficult, and lacks methods with good accuracy. This study aimed to explore the efficacy of indocyanine green fluorescence angiography (ICGA) in intraoperatively assessing wound perfusion and predicting postoperative wound necrosis and clinical outcomes.</p><p><strong>Methods: </strong>A total of 22 patients with orthopaedic oncological diseases were enrolled in this study from August 2021 to December 2022. All patients were deemed to have high risk of postoperative necrosis but normal wound appearance during surgery. ICGA was performed intraoperatively to assess the perfusion status of the wound. A novel system, called the Fluorescence Perfusion Scale (FPS), was proposed, consisting of three types of fluorescence angiography features corresponding to different perfusion statuses. Patient- and provider-related risk factors were analyzed. The relationship between clinical outcomes and FPS types was analyzed.</p><p><strong>Results: </strong>Wound necrosis occurred in ten of 22 patients (46%). According to the FPS, seven patients (32%) showed type 1, seven patients (32%) showed type 2, and eight patients (36%) showed type 3 angiography, respectively. The uni- and multivariate analysis indicated that FPS type 1 or 2 is the only independent risk factor for wound necrosis. The necrosis rate showed a significant difference between FPS types (p<0.001). The rate of reoperation of patients of type 1 was significantly higher than that of type 2 (85% compared 0%, p = 0.005).</p><p><strong>Conclusion: </strong>Wound perfusion in bone and soft-tissue surgery can be assessed by ICGA and graded by the FPS system, which can predict postoperative necrosis and clinical outcomes.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 7","pages":"796-806"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246870/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.67.BJO-2024-0248.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Wound complication is common in bone and soft-tissue tumour surgery. Proper wound healing requires robust blood perfusion. However, intraoperative assessment of perfusion is difficult, and lacks methods with good accuracy. This study aimed to explore the efficacy of indocyanine green fluorescence angiography (ICGA) in intraoperatively assessing wound perfusion and predicting postoperative wound necrosis and clinical outcomes.
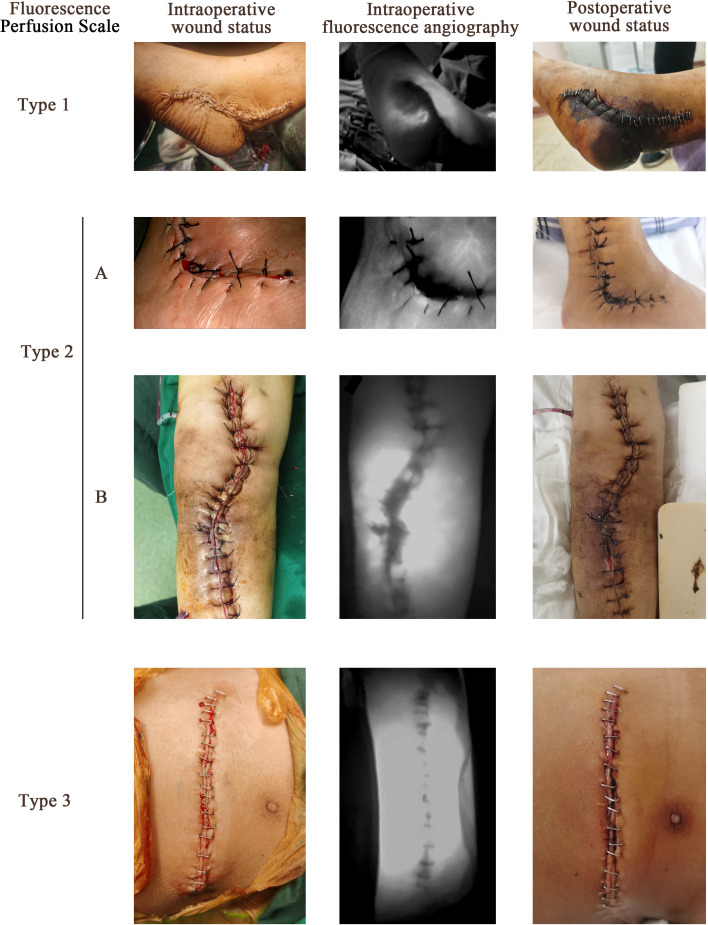
Methods: A total of 22 patients with orthopaedic oncological diseases were enrolled in this study from August 2021 to December 2022. All patients were deemed to have high risk of postoperative necrosis but normal wound appearance during surgery. ICGA was performed intraoperatively to assess the perfusion status of the wound. A novel system, called the Fluorescence Perfusion Scale (FPS), was proposed, consisting of three types of fluorescence angiography features corresponding to different perfusion statuses. Patient- and provider-related risk factors were analyzed. The relationship between clinical outcomes and FPS types was analyzed.
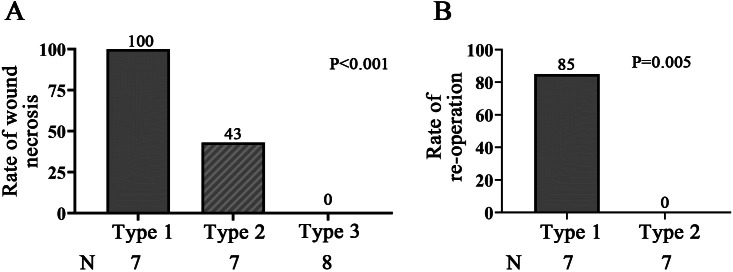
Results: Wound necrosis occurred in ten of 22 patients (46%). According to the FPS, seven patients (32%) showed type 1, seven patients (32%) showed type 2, and eight patients (36%) showed type 3 angiography, respectively. The uni- and multivariate analysis indicated that FPS type 1 or 2 is the only independent risk factor for wound necrosis. The necrosis rate showed a significant difference between FPS types (p<0.001). The rate of reoperation of patients of type 1 was significantly higher than that of type 2 (85% compared 0%, p = 0.005).
Conclusion: Wound perfusion in bone and soft-tissue surgery can be assessed by ICGA and graded by the FPS system, which can predict postoperative necrosis and clinical outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


