Analgesic and Sedative Effect of Fentanyl Versus Dexmedetomidine Infusion in Postoperative Mechanically Ventilated Children After Open Abdominal Surgeries: Randomized Controlled Trial.
{"title":"Analgesic and Sedative Effect of Fentanyl Versus Dexmedetomidine Infusion in Postoperative Mechanically Ventilated Children After Open Abdominal Surgeries: Randomized Controlled Trial.","authors":"Amany Mohamed Abotaleb, Mai Rabie Elsheikh, Khalid Mohamed Elshimy, Mohamed Elsaid AbdelFattah","doi":"10.1155/anrp/9699738","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Optimal sedation and analgesia management in mechanically ventilated (MV) children post-abdominal surgery remain controversial. This study compared the efficacy and safety of fentanyl versus dexmedetomidine infusion in this population. <b>Methods:</b> A randomized, double-blinded study enrolled 54 MV children aged 4-11 years post-open abdominal surgeries. Patients received either fentanyl (1 μg/kg bolus, 1-5 μg/kg/h infusion) in Group F or dexmedetomidine (1 μg/kg bolus, 0.2-0.7 μg/kg/h infusion) in Group D. Hemodynamic parameters, sedation (COMFORT-B scale), pain (FLACC scale), and weaning times were assessed. <b>Results:</b> Group D showed significantly lower mean arterial pressure and heart rates from 6 to 24 h post-intervention (<i>p</i> < 0.05). Oxygen saturation remained similar between groups. Dexmedetomidine provided superior sedation (COMFORT-B: 7 [6-8] vs. 8 [7-8], <i>p</i>=0.022) and analgesia (FLACC: 1 [1-2.5] vs. 2 [2-3], <i>p</i>=0.005). However, dexmedetomidine achieved faster weaning (25.89 ± 2.01 vs. 29.19 ± 1.44 h, <i>p</i> < 0.001) and higher extubation times (51.93 ± 4.84 vs. 43.78 ± 5.32 min, <i>p</i> < 0.001). <b>Conclusions:</b> While dexmedetomidine offered better sedation and pain control, fentanyl facilitated quicker weaning and extubation from MV and better hemodynamics in postoperative MV children after open abdominal surgeries. <b>Trial Registration:</b> ClinicalTrials.gov identifier: NCT06994273.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2025 ","pages":"9699738"},"PeriodicalIF":1.3000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245487/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/anrp/9699738","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
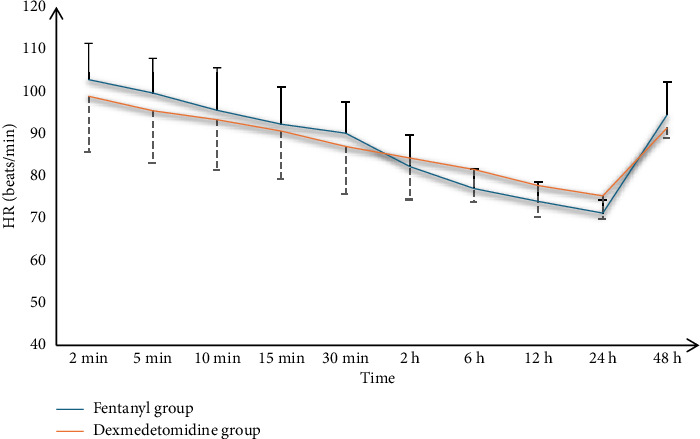
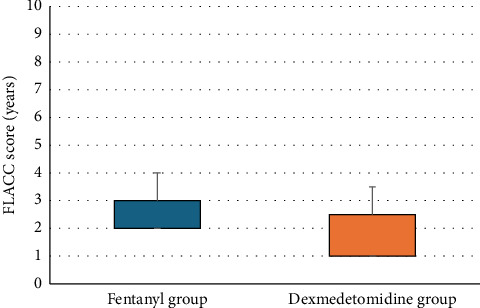
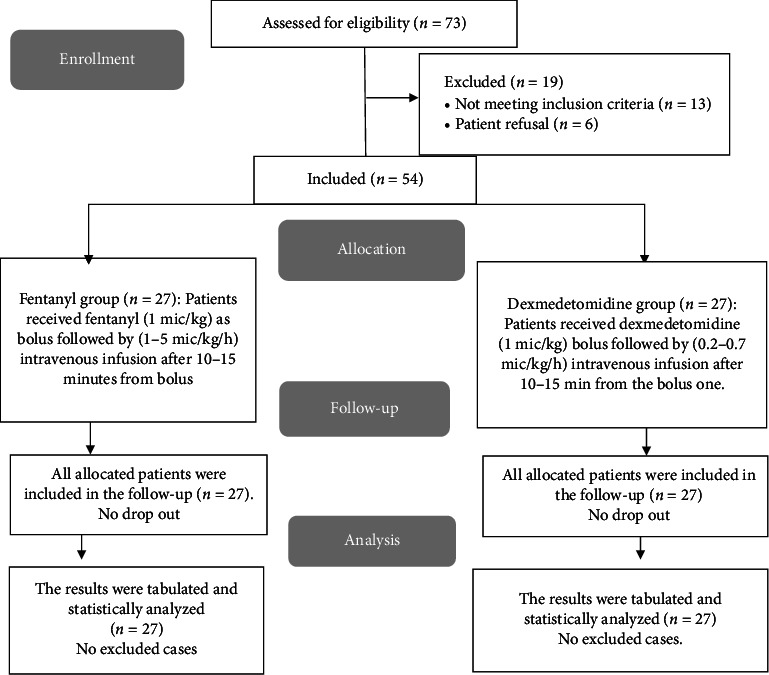
Background: Optimal sedation and analgesia management in mechanically ventilated (MV) children post-abdominal surgery remain controversial. This study compared the efficacy and safety of fentanyl versus dexmedetomidine infusion in this population. Methods: A randomized, double-blinded study enrolled 54 MV children aged 4-11 years post-open abdominal surgeries. Patients received either fentanyl (1 μg/kg bolus, 1-5 μg/kg/h infusion) in Group F or dexmedetomidine (1 μg/kg bolus, 0.2-0.7 μg/kg/h infusion) in Group D. Hemodynamic parameters, sedation (COMFORT-B scale), pain (FLACC scale), and weaning times were assessed. Results: Group D showed significantly lower mean arterial pressure and heart rates from 6 to 24 h post-intervention (p < 0.05). Oxygen saturation remained similar between groups. Dexmedetomidine provided superior sedation (COMFORT-B: 7 [6-8] vs. 8 [7-8], p=0.022) and analgesia (FLACC: 1 [1-2.5] vs. 2 [2-3], p=0.005). However, dexmedetomidine achieved faster weaning (25.89 ± 2.01 vs. 29.19 ± 1.44 h, p < 0.001) and higher extubation times (51.93 ± 4.84 vs. 43.78 ± 5.32 min, p < 0.001). Conclusions: While dexmedetomidine offered better sedation and pain control, fentanyl facilitated quicker weaning and extubation from MV and better hemodynamics in postoperative MV children after open abdominal surgeries. Trial Registration: ClinicalTrials.gov identifier: NCT06994273.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


