João Paulo Machado Bergamaschi, Ariel Falbel Lugão, Rangel Roberto de Assis, Kelsen de Oliveira Teixeira, Fernando Flores de Araújo, Thiago Queiroz Soares, Gustavo Vitelli Depieri, Álvaro Dowling, Robson Cruz de Oliveira, Fernanda Wirth, Fábio da Silva Forti, Helton Luiz Aparecido Defino
{"title":"Transient C5 Palsy After Full-Endoscopic Posterior Cervical Foraminotomy.","authors":"João Paulo Machado Bergamaschi, Ariel Falbel Lugão, Rangel Roberto de Assis, Kelsen de Oliveira Teixeira, Fernando Flores de Araújo, Thiago Queiroz Soares, Gustavo Vitelli Depieri, Álvaro Dowling, Robson Cruz de Oliveira, Fernanda Wirth, Fábio da Silva Forti, Helton Luiz Aparecido Defino","doi":"10.1155/cro/7787076","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Postoperative C5 paralysis is defined as new-onset and/or progressive muscle weakness with mild or no sensory disturbances occurring as a result of probable neuropraxia of the cervical root due to injury during surgery. <b>Case Report:</b> A 40-year-old female patient underwent endoscopic technique for treatment of cervical foraminal stenosis, level C4-C5. The procedure proceeded without incident in the intraoperative period. In the immediate postoperative period, the patient developed a motor deficit, Grade 2 muscle strength of the right deltoid muscle, and right C5 allodynia. Early and multidisciplinary treatment resulted in complete recovery of the neurological deficit and satisfactory evolution of the presented case. <b>Discussion:</b> Although postoperative C5 palsy is one of the most common postoperative complications after multilevel cervical decompression surgery, its exact mechanism remains poorly understood. Despite the various studies in this field and the possible causes described, there is still no absolute confirmation, so the formulation of hypotheses depends on clinical monitoring and postoperative examinations. The indicated treatment depends on the causal suspicion and pathophysiology and ranges from clinical drug therapy to physical therapies and/or rehabilitation. <b>Conclusion:</b> C5 paralysis after endoscopic surgery, although rare, is a potential complication. The likely pathophysiology is multifactorial: anatomic features of C5, manipulation of the root, and use of the bipolar in the foraminal region.</p>","PeriodicalId":30287,"journal":{"name":"Case Reports in Orthopedics","volume":"2025 ","pages":"7787076"},"PeriodicalIF":0.6000,"publicationDate":"2025-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240654/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/cro/7787076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
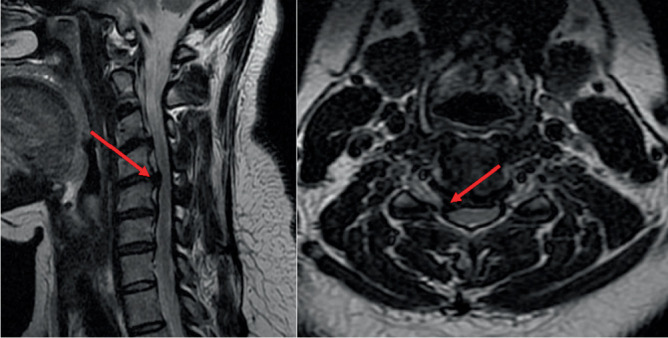
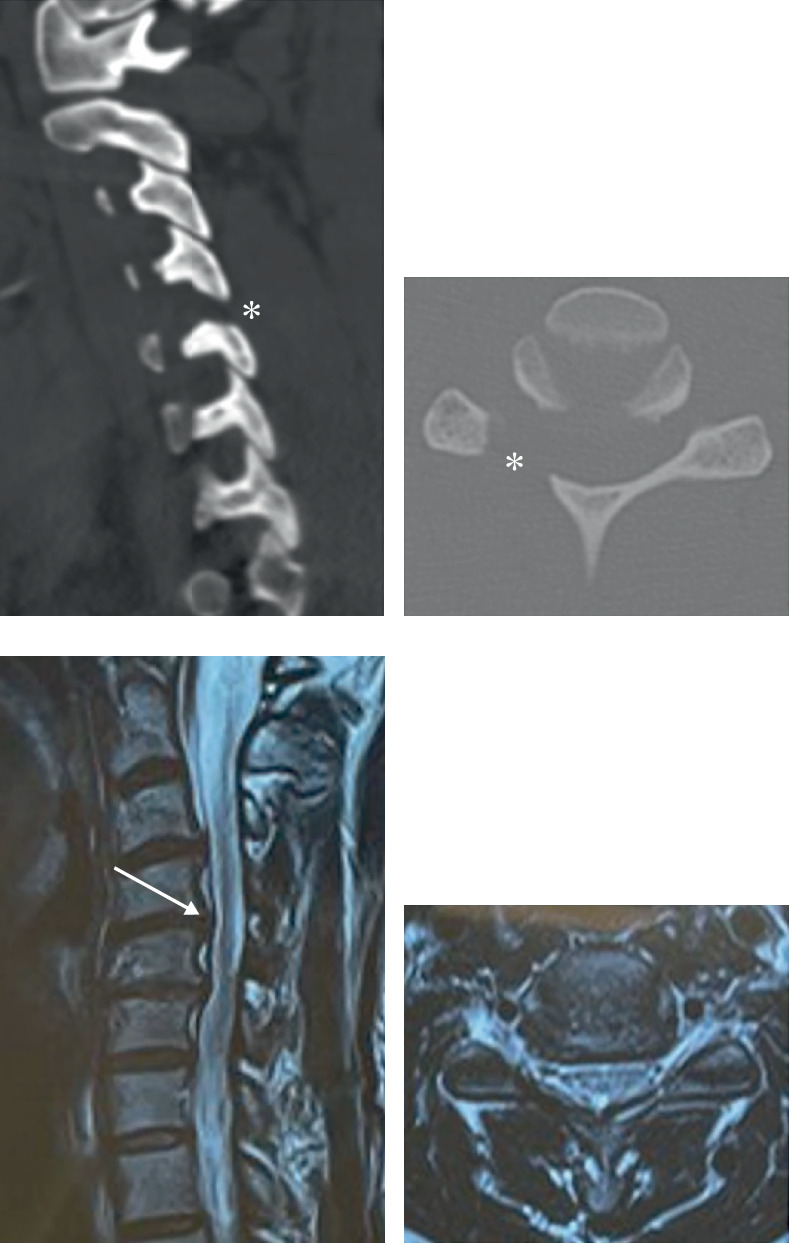
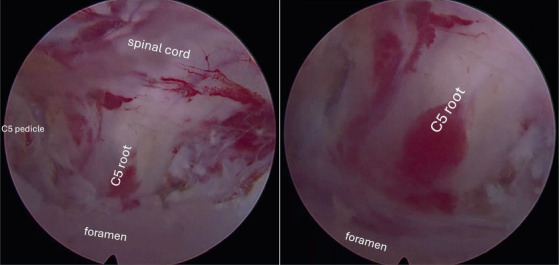
Introduction: Postoperative C5 paralysis is defined as new-onset and/or progressive muscle weakness with mild or no sensory disturbances occurring as a result of probable neuropraxia of the cervical root due to injury during surgery. Case Report: A 40-year-old female patient underwent endoscopic technique for treatment of cervical foraminal stenosis, level C4-C5. The procedure proceeded without incident in the intraoperative period. In the immediate postoperative period, the patient developed a motor deficit, Grade 2 muscle strength of the right deltoid muscle, and right C5 allodynia. Early and multidisciplinary treatment resulted in complete recovery of the neurological deficit and satisfactory evolution of the presented case. Discussion: Although postoperative C5 palsy is one of the most common postoperative complications after multilevel cervical decompression surgery, its exact mechanism remains poorly understood. Despite the various studies in this field and the possible causes described, there is still no absolute confirmation, so the formulation of hypotheses depends on clinical monitoring and postoperative examinations. The indicated treatment depends on the causal suspicion and pathophysiology and ranges from clinical drug therapy to physical therapies and/or rehabilitation. Conclusion: C5 paralysis after endoscopic surgery, although rare, is a potential complication. The likely pathophysiology is multifactorial: anatomic features of C5, manipulation of the root, and use of the bipolar in the foraminal region.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


