Could Plasma Glucose (PG) Increment (PG%) Expand the Clinical Weight of OGTT? Preliminary Findings in 19 TDT Patients (β-TDT) with Normal Glucose Tolerance.
Vincenzo de Sanctis, Ashraf T Soliman, Shahina Daar, Ploutarchos Tzoulis, Christos Kattamis
{"title":"Could Plasma Glucose (PG) Increment (PG%) Expand the Clinical Weight of OGTT? Preliminary Findings in 19 TDT Patients (β-TDT) with Normal Glucose Tolerance.","authors":"Vincenzo de Sanctis, Ashraf T Soliman, Shahina Daar, Ploutarchos Tzoulis, Christos Kattamis","doi":"10.4084/MJHID.2025.050","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Worldwide, glucose dysregulation (GD) and diabetes mellitus are common complications in transfusion-dependent β-thalassemia (β-TDT) patients. Impaired insulin sensitivity and insulin secretion are both involved in the deterioration of glucose tolerance from a normal to a glucose-intolerant state.</p><p><strong>Objective: </strong>The main aim of the present study was to evaluate the plasma glucose (PG) increment (PG %) retrospectively at two h during oral glucose tolerance test (OGTT) over fasting plasma (FPG) concentration as a simple parameter to recognize early β-cell dysfunction in normoglycemic β-TDT patients with NGT and different severities of iron overload (IOL).</p><p><strong>Patients and methods: </strong>A total of 19 β-TDT young adult patients with normal OGTT were re-evaluated according to the American Diabetes Association (ADA) guidelines. Venous blood samples were collected at baseline and at 30, 60, and 120 minutes to determine PG (mg/dL) and insulin concentrations (μIU/mL). The time required for the PG concentration to return to the fasting level was calculated by computing the percentage increment of 2-h PG with respect to FPG (PG%), using the formula [(2-h PG-FPG)/FPG]x 100. The early phase of insulin secretion (IGI) and sensitivity were assessed by validated surrogate indices calculated from parameters obtained during the four-point OGTT.</p><p><strong>Results: </strong>The mean age of patients was 30.3 ± 5.7 (range: 23.10-44.3). The mean ± SD, median, and range of PG% increment between 2 h-PG and FPG were 35.5 ± 20.2, 38.7, and 0 - 68.2 mg/dL, respectively. The PG% increment was negatively correlated to the patient's age, FPG, and IGI, and positively correlated with 2-h PG post-glucose load. IGI was negatively correlated with 1-h and 2-h PG after post-glucose load and positively correlated with oral disposition index (oDI).</p><p><strong>Conclusions: </strong>The PG% increment is a simple, useful screening parameter that can expand the clinical weight of OGTT and can provide valuable metabolic information on β-cell dysfunction.</p>","PeriodicalId":18498,"journal":{"name":"Mediterranean Journal of Hematology and Infectious Diseases","volume":"17 1","pages":"e2025050"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240246/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediterranean Journal of Hematology and Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4084/MJHID.2025.050","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Worldwide, glucose dysregulation (GD) and diabetes mellitus are common complications in transfusion-dependent β-thalassemia (β-TDT) patients. Impaired insulin sensitivity and insulin secretion are both involved in the deterioration of glucose tolerance from a normal to a glucose-intolerant state.
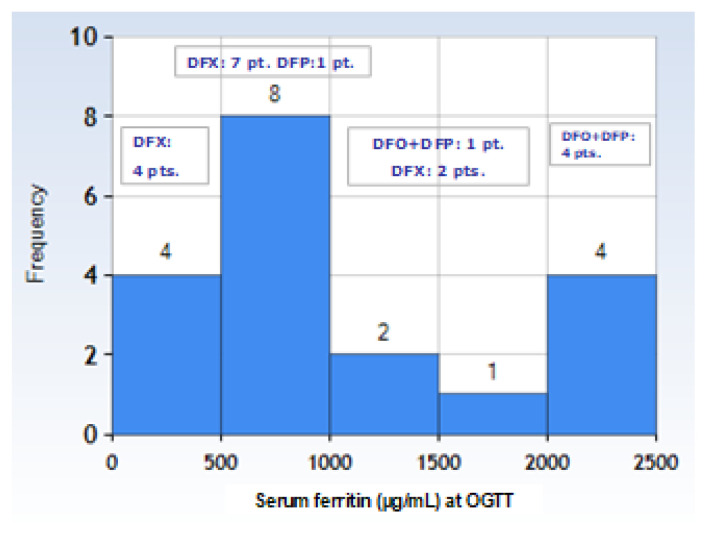
Objective: The main aim of the present study was to evaluate the plasma glucose (PG) increment (PG %) retrospectively at two h during oral glucose tolerance test (OGTT) over fasting plasma (FPG) concentration as a simple parameter to recognize early β-cell dysfunction in normoglycemic β-TDT patients with NGT and different severities of iron overload (IOL).
Patients and methods: A total of 19 β-TDT young adult patients with normal OGTT were re-evaluated according to the American Diabetes Association (ADA) guidelines. Venous blood samples were collected at baseline and at 30, 60, and 120 minutes to determine PG (mg/dL) and insulin concentrations (μIU/mL). The time required for the PG concentration to return to the fasting level was calculated by computing the percentage increment of 2-h PG with respect to FPG (PG%), using the formula [(2-h PG-FPG)/FPG]x 100. The early phase of insulin secretion (IGI) and sensitivity were assessed by validated surrogate indices calculated from parameters obtained during the four-point OGTT.
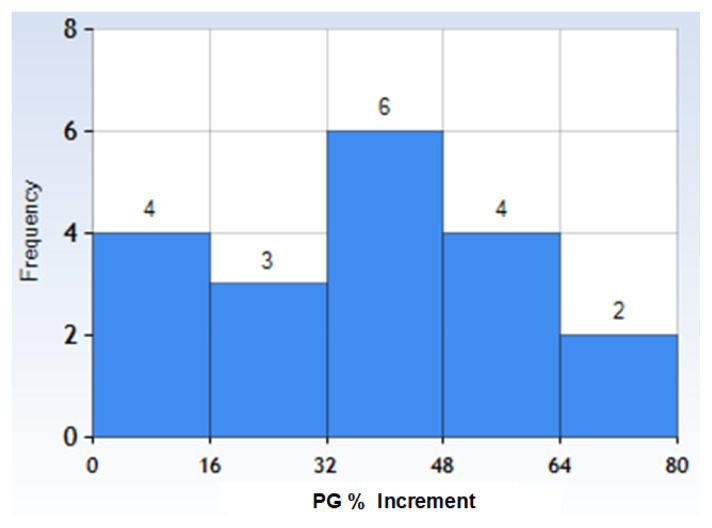
Results: The mean age of patients was 30.3 ± 5.7 (range: 23.10-44.3). The mean ± SD, median, and range of PG% increment between 2 h-PG and FPG were 35.5 ± 20.2, 38.7, and 0 - 68.2 mg/dL, respectively. The PG% increment was negatively correlated to the patient's age, FPG, and IGI, and positively correlated with 2-h PG post-glucose load. IGI was negatively correlated with 1-h and 2-h PG after post-glucose load and positively correlated with oral disposition index (oDI).
Conclusions: The PG% increment is a simple, useful screening parameter that can expand the clinical weight of OGTT and can provide valuable metabolic information on β-cell dysfunction.
期刊介绍:
Reciprocal interdependence between infectious and hematologic diseases (malignant and non-malignant) is well known. This relationship is particularly evident in Mediterranean countries. Parasitosis as Malaria, Leishmaniosis, B Hookworms, Teniasis, very common in the southeast Mediterranean area, infect about a billion people and manifest prevalently with anemia so that they are usually diagnosed mostly by experienced hematologist on blood or bone marrow smear. On the other hand, infections are also a significant problem in patients affected by hematological malignancies. The blood is the primary vector of HIV infection, which otherwise manifest with symptoms related to a reduction in T lymphocytes. In turn, infections can favor the insurgency of hematological malignancies. The causative relationship between Epstein-Barr virus infection, Helicobacter pylori, hepatitis C virus, HIV and lymphoproliferative diseases is well known.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


