Samuel B Hayworth, Desalyn L Johnson, Erinn O Schmit
{"title":"Posterior Reversible Encephalopathy Syndrome Leading to Diagnosis of Acute Postinfectious Glomerulonephritis in a Pediatric Patient: A Case Report.","authors":"Samuel B Hayworth, Desalyn L Johnson, Erinn O Schmit","doi":"10.1155/crpe/9946572","DOIUrl":null,"url":null,"abstract":"<p><p><b>History:</b> An 8-year-old previously healthy female presented to the emergency department after new-onset seizure activity. Three days prior, she experienced severe headaches and rash over her left lower extremity. She developed nonbilious, nonbloody emesis on the day prior to admission. The morning of presentation, she was found unresponsive, exhibiting right gaze deviation and clenched jaw concerning for seizure activity. Further history revealed recent Group A streptococcal pharyngitis, which had been treated with a 10-day regimen of amoxicillin. During this time, her mother reported decreased oral intake but normal urinary output, without dysuria or hematuria. <b>Physical Examination:</b> Vital signs were notable for temperature of 101.7 degrees Fahrenheit, heart rate of 100 beats per minute, blood pressure of 167/97, respiratory rate of 28, and oxygen saturation of 96% on room air. The patient was drowsy but arousable. Her neck was supple without evidence of meningismus. A skin exam revealed an erythematous, crusting rash, resembling contact dermatitis on the left lower extremity below the knee. The patient was somnolent but oriented to self and able to follow simple commands. Cranial nerves II-XII were intact bilaterally. Sensory, motor, and coordination were unremarkable. <b>Laboratory, Imaging, and Procedures:</b> Laboratory findings included leukocytosis, microscopic hematuria, decreased C3 and C4 levels, and positive antistreptolysin O (ASO) titers. A lumbar puncture was conducted with unremarkable cerebrospinal fluid (CSF) indices. Imaging revealed hypoattenuation in the occipital lobes on computed tomography (CT) venogram and hyperintensities in bilateral occipital lobes on magnetic resonance imaging (MRI) T2 fluid-attenuated inversion recovery (FLAIR) sequences, consistent with posterior reversible encephalopathy syndrome (PRES). <b>Discussion:</b> PRES in pediatric patients has been associated with a variety of conditions including hypertension (idiopathic or secondary), renal disorders, autoimmune disorders, and hematologic or oncologic conditions. However, PRES secondary to acute postinfectious glomerulonephritis (PIGN) is rare. Hematuria on the urinalysis led to obtaining complement levels, and further elucidation of history helped to narrow the differential to PIGN due to streptococcal infection with confirmatory positive ASO antibody titer. This case highlights a rare sequala of a commonly seen pediatric infection.</p>","PeriodicalId":9623,"journal":{"name":"Case Reports in Pediatrics","volume":"2025 ","pages":"9946572"},"PeriodicalIF":0.5000,"publicationDate":"2025-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240652/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crpe/9946572","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
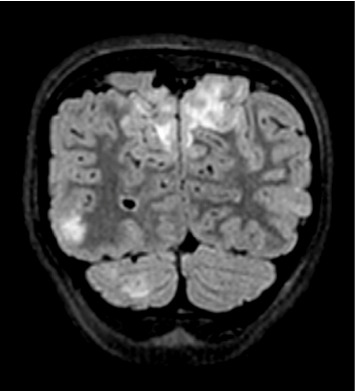
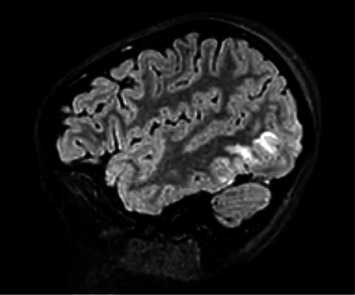
History: An 8-year-old previously healthy female presented to the emergency department after new-onset seizure activity. Three days prior, she experienced severe headaches and rash over her left lower extremity. She developed nonbilious, nonbloody emesis on the day prior to admission. The morning of presentation, she was found unresponsive, exhibiting right gaze deviation and clenched jaw concerning for seizure activity. Further history revealed recent Group A streptococcal pharyngitis, which had been treated with a 10-day regimen of amoxicillin. During this time, her mother reported decreased oral intake but normal urinary output, without dysuria or hematuria. Physical Examination: Vital signs were notable for temperature of 101.7 degrees Fahrenheit, heart rate of 100 beats per minute, blood pressure of 167/97, respiratory rate of 28, and oxygen saturation of 96% on room air. The patient was drowsy but arousable. Her neck was supple without evidence of meningismus. A skin exam revealed an erythematous, crusting rash, resembling contact dermatitis on the left lower extremity below the knee. The patient was somnolent but oriented to self and able to follow simple commands. Cranial nerves II-XII were intact bilaterally. Sensory, motor, and coordination were unremarkable. Laboratory, Imaging, and Procedures: Laboratory findings included leukocytosis, microscopic hematuria, decreased C3 and C4 levels, and positive antistreptolysin O (ASO) titers. A lumbar puncture was conducted with unremarkable cerebrospinal fluid (CSF) indices. Imaging revealed hypoattenuation in the occipital lobes on computed tomography (CT) venogram and hyperintensities in bilateral occipital lobes on magnetic resonance imaging (MRI) T2 fluid-attenuated inversion recovery (FLAIR) sequences, consistent with posterior reversible encephalopathy syndrome (PRES). Discussion: PRES in pediatric patients has been associated with a variety of conditions including hypertension (idiopathic or secondary), renal disorders, autoimmune disorders, and hematologic or oncologic conditions. However, PRES secondary to acute postinfectious glomerulonephritis (PIGN) is rare. Hematuria on the urinalysis led to obtaining complement levels, and further elucidation of history helped to narrow the differential to PIGN due to streptococcal infection with confirmatory positive ASO antibody titer. This case highlights a rare sequala of a commonly seen pediatric infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


