{"title":"Evaluating implementation preparedness for suicide screening and referral in a Nepali emergency department: A mixed-methods study.","authors":"Anmol P Shrestha, Roshana Shrestha, Ajay Risal, Renu Shakya, Kripa Sigdel, Riya Bajracharya, Pratiksha Paudel, Divya Gumudavelly, Emilie Egger, Sophia Zhuang, Lakshmi Vijayakumar, Ashley Hagaman","doi":"10.1177/26334895251343644","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Most research on appropriate, feasible, and effective suicide screening has excluded research conducted in non-Western and low-income settings. This study explores preparedness and co-designing a suicide screening and referral intervention in a Nepali emergency department (ED) using the Consolidated Framework for Implementation Research (CFIR).</p><p><strong>Method: </strong>To assess implementation readiness and context, we conducted eight key informant interviews and four focus-group discussions with clinical staff along with 3 months of embedded ethnography. We also assessed clinical staff (<i>n</i> = 26) knowledge, attitudes, current practices, confidence, and institutional priorities surrounding implementing suicide screening using structured questionnaires. Qualitative analysis used CFIR to assess feasibility, acceptability, and necessary implementation strategies for a suicide screening intervention within the context of this resource-strained ED. We report descriptive statistics of quantitative findings using a convergent analytic mixed-methods approach.</p><p><strong>Results: </strong>Qualitatively, clinicians expressed hopelessness and reservations surrounding ED programs to prevent suicide given important system and social barriers. Additionally, they doubted their ability to meaningfully overcome broader structural issues in their patients' lives (e.g., poverty and family tension) that they believed more directly determined suicidal behavior and thwarted help seeking. They discussed practical and emotional motivators for doing suicide prevention work, which highlighted departmental leadership and deep teamwork that motivated action despite wider societal myths that suicide cannot easily be prevented. Quantitative assessments largely supported these findings, indicating shared beliefs that suicide prevention was important and supported by leadership. However, providers frequently endorsed suicide myths and noted barriers including difficult interdepartmental collaboration, limited confidence in suicide prevention communication and suicide screening.</p><p><strong>Conclusions: </strong>In under-resourced settings, staff must contend with competing responsibilities and complex structural causes of suicide and barriers to treatment. These can impede implementation of suicide screening interventions and must be integrated into the co-design of implementation strategy selection and deployment.</p><p><strong>Trial registration: </strong>NCT06094959 clinicaltrials.gov.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"6 ","pages":"26334895251343644"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235230/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895251343644","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Most research on appropriate, feasible, and effective suicide screening has excluded research conducted in non-Western and low-income settings. This study explores preparedness and co-designing a suicide screening and referral intervention in a Nepali emergency department (ED) using the Consolidated Framework for Implementation Research (CFIR).
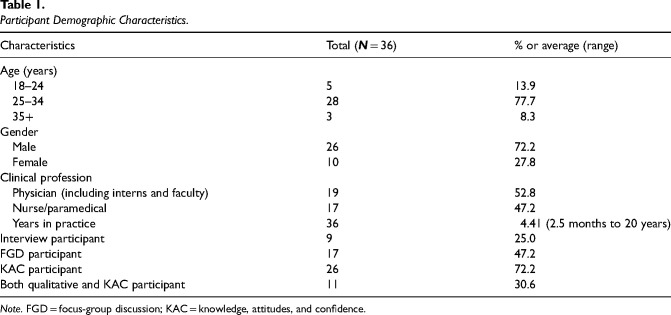
Method: To assess implementation readiness and context, we conducted eight key informant interviews and four focus-group discussions with clinical staff along with 3 months of embedded ethnography. We also assessed clinical staff (n = 26) knowledge, attitudes, current practices, confidence, and institutional priorities surrounding implementing suicide screening using structured questionnaires. Qualitative analysis used CFIR to assess feasibility, acceptability, and necessary implementation strategies for a suicide screening intervention within the context of this resource-strained ED. We report descriptive statistics of quantitative findings using a convergent analytic mixed-methods approach.
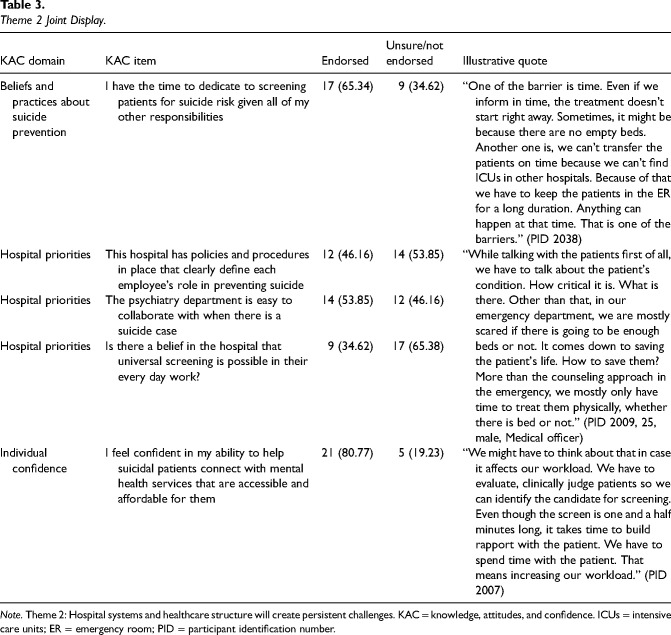
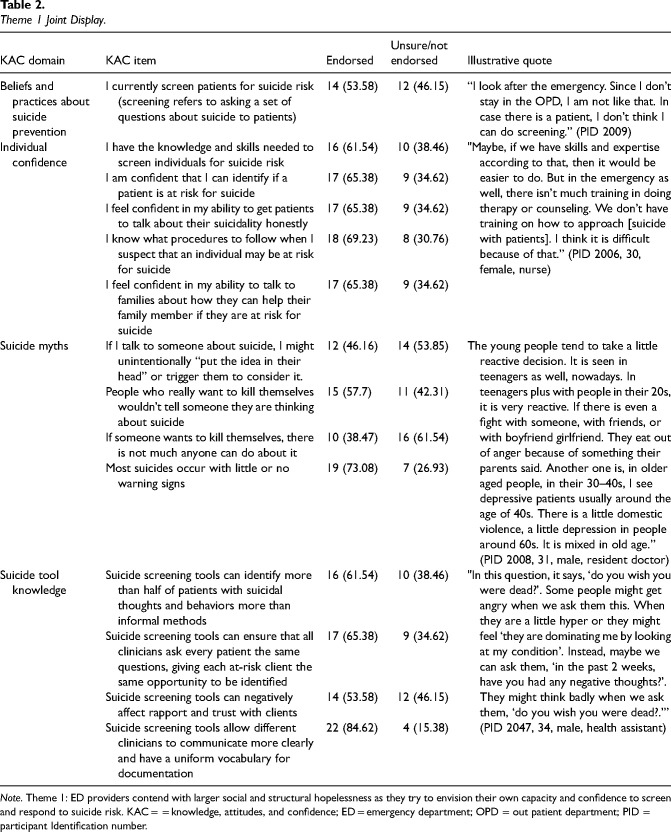
Results: Qualitatively, clinicians expressed hopelessness and reservations surrounding ED programs to prevent suicide given important system and social barriers. Additionally, they doubted their ability to meaningfully overcome broader structural issues in their patients' lives (e.g., poverty and family tension) that they believed more directly determined suicidal behavior and thwarted help seeking. They discussed practical and emotional motivators for doing suicide prevention work, which highlighted departmental leadership and deep teamwork that motivated action despite wider societal myths that suicide cannot easily be prevented. Quantitative assessments largely supported these findings, indicating shared beliefs that suicide prevention was important and supported by leadership. However, providers frequently endorsed suicide myths and noted barriers including difficult interdepartmental collaboration, limited confidence in suicide prevention communication and suicide screening.
Conclusions: In under-resourced settings, staff must contend with competing responsibilities and complex structural causes of suicide and barriers to treatment. These can impede implementation of suicide screening interventions and must be integrated into the co-design of implementation strategy selection and deployment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


