{"title":"Comparison of EuroSCORE II and STS Risk Scoring Systems in Patients who Underwent Open-heart Surgery.","authors":"Erkam Saka, Esin Öztürk, Aslıhan Esra Yüksel, Nüzhet Seden Kocabaş","doi":"10.4274/TJAR.2025.241778","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>In the present study, European Cardiac Operative Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgery (STS) risk scoring systems were used to predict mortality in patients who underwent various types of open-heart surgery, including coronary artery bypass grafting, aortic valve replacement, mitral valve replacement, and combined valve surgery with coronary artery bypass grafting, in the cardiovascular surgery operating room. The aim was to compare risk assessment systems regarding their clinical applicability.</p><p><strong>Methods: </strong>A total of 469 patients, 141 (30.1%) female and 328 (69.9%) male, were included in the study. All risk factors were retrospectively recorded according to the EuroSCORE II and STS risk assessment systems. Statistical analysis was performed using the receiver operating characteristic (ROC) curve. Predicted and actual mortality rates were compared for each risk-scoring system.</p><p><strong>Results: </strong>When the ability of the EuroSCORE and STS risk classifications to predict mortality was analyzed using the ROC curve, the area under the curve for the EuroSCORE II risk score was 78.3% (<i>P</i> < 0.001), while the area under the curve for the STS risk score was 82.3% (<i>P</i> < 0.001). In our study, the STS scoring system was found to have a greater predictive value than EuroSCORE II. When the patients' observed and expected mortality rates were examined according to the EuroSCORE II and STS risk scores, no statistically significant relationship was found between the expected and observed mortality rates for each risk group.</p><p><strong>Conclusion: </strong>In our study, the STS risk scoring system was found to be more accurate in predicting in-hospital mortality than the EuroSCORE. However, there was no statistically significant difference between the expected and observed mortality rates in either risk-scoring system. There is no consensus in the literature regarding which scoring system is more effective. More studies from different societies are needed.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":" ","pages":"163-169"},"PeriodicalIF":0.9000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288423/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2025.241778","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: In the present study, European Cardiac Operative Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgery (STS) risk scoring systems were used to predict mortality in patients who underwent various types of open-heart surgery, including coronary artery bypass grafting, aortic valve replacement, mitral valve replacement, and combined valve surgery with coronary artery bypass grafting, in the cardiovascular surgery operating room. The aim was to compare risk assessment systems regarding their clinical applicability.
Methods: A total of 469 patients, 141 (30.1%) female and 328 (69.9%) male, were included in the study. All risk factors were retrospectively recorded according to the EuroSCORE II and STS risk assessment systems. Statistical analysis was performed using the receiver operating characteristic (ROC) curve. Predicted and actual mortality rates were compared for each risk-scoring system.
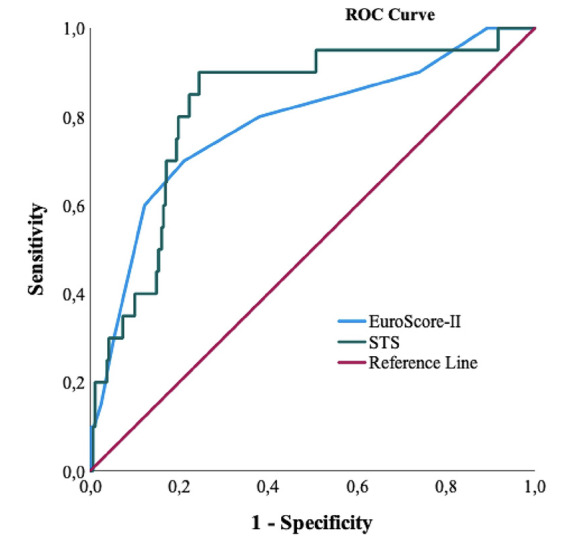
Results: When the ability of the EuroSCORE and STS risk classifications to predict mortality was analyzed using the ROC curve, the area under the curve for the EuroSCORE II risk score was 78.3% (P < 0.001), while the area under the curve for the STS risk score was 82.3% (P < 0.001). In our study, the STS scoring system was found to have a greater predictive value than EuroSCORE II. When the patients' observed and expected mortality rates were examined according to the EuroSCORE II and STS risk scores, no statistically significant relationship was found between the expected and observed mortality rates for each risk group.
Conclusion: In our study, the STS risk scoring system was found to be more accurate in predicting in-hospital mortality than the EuroSCORE. However, there was no statistically significant difference between the expected and observed mortality rates in either risk-scoring system. There is no consensus in the literature regarding which scoring system is more effective. More studies from different societies are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


