Unveiling the best immune checkpoint inhibitor-based therapy for metastatic renal cell carcinoma in the first-line setting: an updated systematic review and Bayesian network analysis.
{"title":"Unveiling the best immune checkpoint inhibitor-based therapy for metastatic renal cell carcinoma in the first-line setting: an updated systematic review and Bayesian network analysis.","authors":"Junpeng Wang, Xin Li, Mengjun Li, Qingyuan Liu, Zixuan Xie, Xiaotian Si, Lei Yang, Zhifeng Wang, Degang Ding","doi":"10.1177/17588359251353259","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitor (ICI)-based combination therapies have been recommended as first-line options for metastatic renal cell carcinoma (mRCC); however, no head-to-head randomized controlled trials (RCTs) have compared all existing ICI-based therapies.</p><p><strong>Objective: </strong>We aimed to analyze the updated data to compare the efficacy of all available ICI-based options for mRCC.</p><p><strong>Design: </strong>A systematic review and Bayesian network analysis.</p><p><strong>Data sources and methods: </strong>A systematic literature search was undertaken up to September 15, 2024, and subsequent analysis was performed using a Bayesian fixed-effect model.</p><p><strong>Results: </strong>This study included 30 RCTs involving 14,959 patients. The results revealed that nivolumab plus cabozantinib (hazard ratio (HR): 0.77; 95% credible interval (CrI): 0.63-0.93), pembrolizumab plus lenvatinib (HR: 0.79; 95% CrI: 0.64-0.99), toripalimab plus axitinib (HR: 0.62; 95% CrI: 0.42-0.97), nivolumab plus ipilimumab (HR: 0.72; 95% CrI: 0.62-0.84), pembrolizumab plus axitinib (HR: 0.84; 95% CrI: 0.71-0.98), and avelumab plus axitinib (HR: 0.79; 95% CrI: 0.64-0.98) were significantly more effective than sunitinib for overall survival (OS). Most ICI-based combination treatments resulted in fewer or similar high-grade adverse events compared to sunitinib, except for pembrolizumab plus lenvatinib. For favorable-risk patients, ICI-based combination therapies were not more effective than sunitinib in OS, while six ICI-based combination therapies were associated with significantly improved OS compared to sunitinib for intermediate-risk or poor-risk patients.</p><p><strong>Conclusion: </strong>Our findings demonstrated that combination therapies including nivolumab plus cabozantinib, pembrolizumab plus lenvatinib, toripalimab plus axitinib, nivolumab plus ipilimumab, pembrolizumab plus axitinib, and avelumab plus axitinib significantly improved OS versus sunitinib. For subgroup analysis, ICI-based combination therapies exhibited significant advantages over sunitinib for intermediate-risk or poor-risk patients, while such advantages were diminished in treating favorable-risk patients.</p>","PeriodicalId":23053,"journal":{"name":"Therapeutic Advances in Medical Oncology","volume":"17 ","pages":"17588359251353259"},"PeriodicalIF":4.2000,"publicationDate":"2025-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235238/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Medical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17588359251353259","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Immune checkpoint inhibitor (ICI)-based combination therapies have been recommended as first-line options for metastatic renal cell carcinoma (mRCC); however, no head-to-head randomized controlled trials (RCTs) have compared all existing ICI-based therapies.
Objective: We aimed to analyze the updated data to compare the efficacy of all available ICI-based options for mRCC.
Design: A systematic review and Bayesian network analysis.
Data sources and methods: A systematic literature search was undertaken up to September 15, 2024, and subsequent analysis was performed using a Bayesian fixed-effect model.
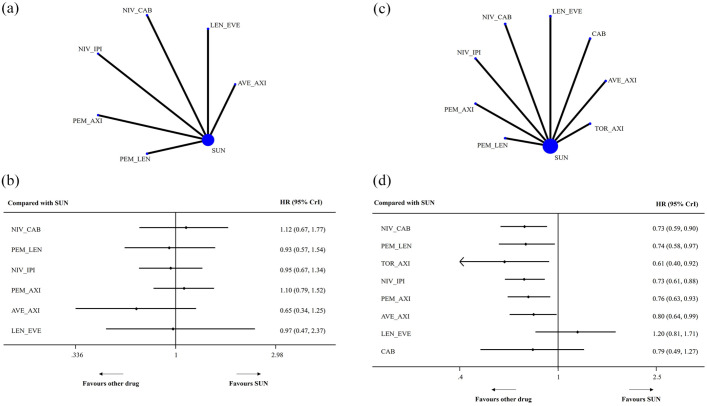
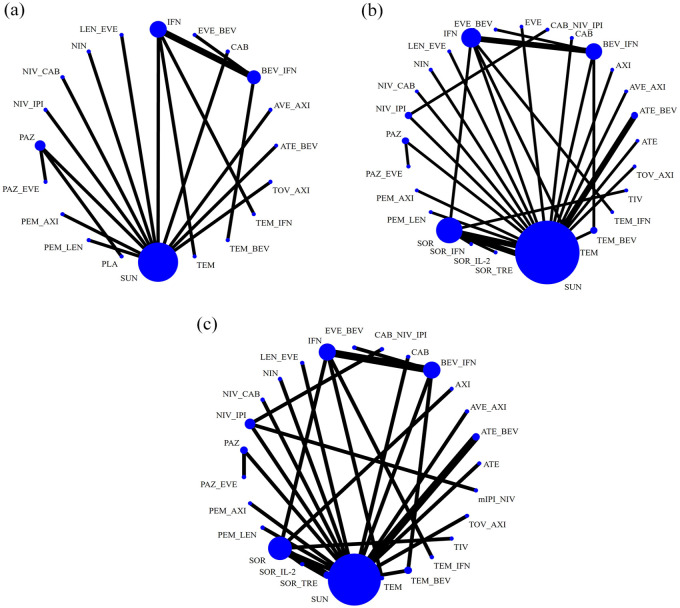
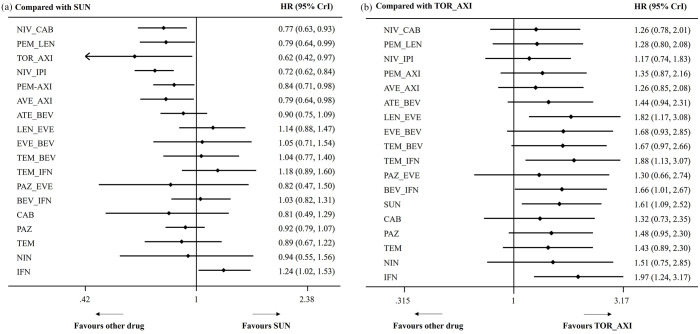
Results: This study included 30 RCTs involving 14,959 patients. The results revealed that nivolumab plus cabozantinib (hazard ratio (HR): 0.77; 95% credible interval (CrI): 0.63-0.93), pembrolizumab plus lenvatinib (HR: 0.79; 95% CrI: 0.64-0.99), toripalimab plus axitinib (HR: 0.62; 95% CrI: 0.42-0.97), nivolumab plus ipilimumab (HR: 0.72; 95% CrI: 0.62-0.84), pembrolizumab plus axitinib (HR: 0.84; 95% CrI: 0.71-0.98), and avelumab plus axitinib (HR: 0.79; 95% CrI: 0.64-0.98) were significantly more effective than sunitinib for overall survival (OS). Most ICI-based combination treatments resulted in fewer or similar high-grade adverse events compared to sunitinib, except for pembrolizumab plus lenvatinib. For favorable-risk patients, ICI-based combination therapies were not more effective than sunitinib in OS, while six ICI-based combination therapies were associated with significantly improved OS compared to sunitinib for intermediate-risk or poor-risk patients.
Conclusion: Our findings demonstrated that combination therapies including nivolumab plus cabozantinib, pembrolizumab plus lenvatinib, toripalimab plus axitinib, nivolumab plus ipilimumab, pembrolizumab plus axitinib, and avelumab plus axitinib significantly improved OS versus sunitinib. For subgroup analysis, ICI-based combination therapies exhibited significant advantages over sunitinib for intermediate-risk or poor-risk patients, while such advantages were diminished in treating favorable-risk patients.
期刊介绍:
Therapeutic Advances in Medical Oncology is an open access, peer-reviewed journal delivering the highest quality articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of cancer. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in medical oncology, providing a forum in print and online for publishing the highest quality articles in this area. This journal is a member of the Committee on Publication Ethics (COPE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


