Cost-Effectiveness of Pembrolizumab Monotherapy for High Programmed Death Ligand 1 Advanced or Metastatic Non-small Cell Lung Cancer Depends on Long-Term Survivors.
Zakile A Mfumbilwa, Janneke A Wilschut, Harry J M Groen, Valesca P Retèl, Bram Ramaekers, Manuela Joore, Veerle M H Coupé
{"title":"Cost-Effectiveness of Pembrolizumab Monotherapy for High Programmed Death Ligand 1 Advanced or Metastatic Non-small Cell Lung Cancer Depends on Long-Term Survivors.","authors":"Zakile A Mfumbilwa, Janneke A Wilschut, Harry J M Groen, Valesca P Retèl, Bram Ramaekers, Manuela Joore, Veerle M H Coupé","doi":"10.1007/s40261-025-01456-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pembrolizumab shows effectiveness in treating metastatic non-small cell lung cancer (metNSCLC), with a subgroup of patients experiencing long-term survival (LTS) benefits. The existence of a LTS subgroup may influence the cost-effectiveness of pembrolizumab monotherapy compared with platinum-based chemotherapy. This study aims to assess the potential implications of such a subgroup on the cost-effectiveness for patients with non-squamous metNSCLC and PD-L1 ≥ 50% who are ineligible for targeted therapies.</p><p><strong>Methods: </strong>This study used a decision analytic model based on Dutch real-world data (2008-2014). Two strategies were simulated: (1) a chemotherapy strategy: patients receive chemotherapy in the first-, second-, and third-line; and (2) a pembrolizumab strategy: patients receive first-line pembrolizumab followed by chemotherapy for those progressing to second- and third-lines. The pembrolizumab strategy is evaluated with and without the assumption that there is a LTS subgroup. The LTS subgroup is assumed to be free from metNSCLC-related progression after treatment. Costs (2022 €), including drug costs, other direct medical costs, family costs, and healthcare costs in life years gained, are considered from first-line treatment to death. Effects are measured in quality-adjusted life years (QALYs). The incremental cost-effectiveness ratio (ICER) is assessed using an €80,000/QALY threshold. Threshold analyses are performed on the size and mortality rate of the LTS subgroup and on the price of pembrolizumab.</p><p><strong>Results: </strong>QALYs per patient were 0.65 for chemotherapy, 1.24 for pembrolizumab without LTS, and 3.52 for pembrolizumab with LTS. Average costs per patient were €58,800 for chemotherapy, €154,600 for pembrolizumab without LTS, and €178,600 for pembrolizumab with LTS. Pembrolizumab without LTS was not cost-effective compared with chemotherapy (ICER €167,600/QALY), but pembrolizumab with LTS (30% of simulated population) was cost effective (ICER of €43,100/QALY). Threshold analyses showed that a LTS subgroup size of at least 10% or halving the price of pembrolizumab was needed for pembrolizumab to be cost-effective.</p><p><strong>Conclusions: </strong>Pembrolizumab is a cost-effective first-line treatment for patients with metNSCLC and PD-L1 ≥ 50% in the Netherlands when at least 10% of patients are long-term survivors. Without long-term survivors, this treatment is not cost-effective. Therefore, it is crucial to consider long-term survivors in assessing the cost-effectiveness of immunotherapy in metNSCLC.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"583-598"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12307520/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40261-025-01456-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pembrolizumab shows effectiveness in treating metastatic non-small cell lung cancer (metNSCLC), with a subgroup of patients experiencing long-term survival (LTS) benefits. The existence of a LTS subgroup may influence the cost-effectiveness of pembrolizumab monotherapy compared with platinum-based chemotherapy. This study aims to assess the potential implications of such a subgroup on the cost-effectiveness for patients with non-squamous metNSCLC and PD-L1 ≥ 50% who are ineligible for targeted therapies.
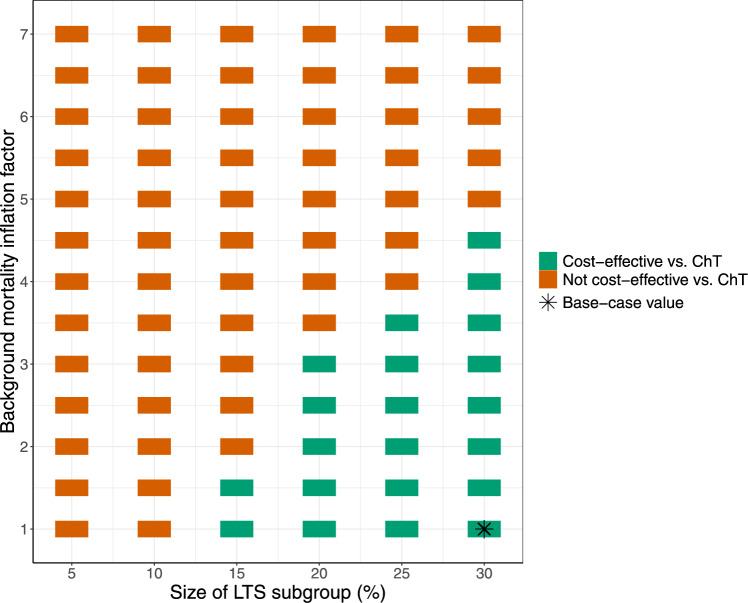
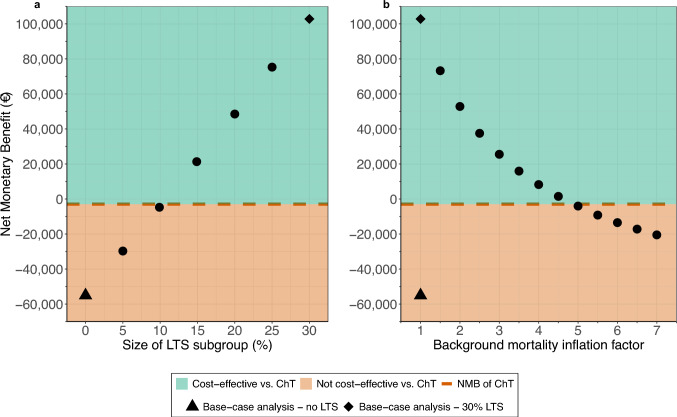
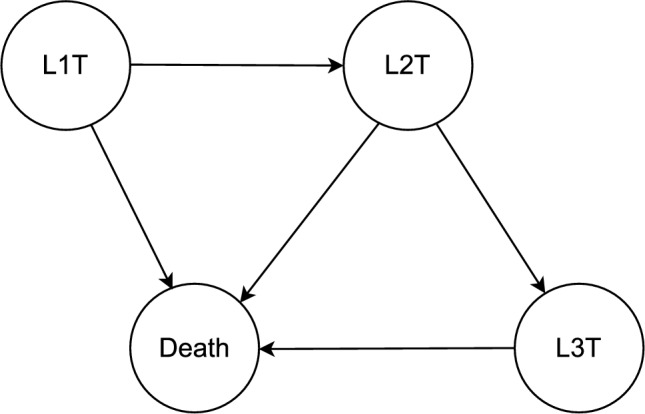
Methods: This study used a decision analytic model based on Dutch real-world data (2008-2014). Two strategies were simulated: (1) a chemotherapy strategy: patients receive chemotherapy in the first-, second-, and third-line; and (2) a pembrolizumab strategy: patients receive first-line pembrolizumab followed by chemotherapy for those progressing to second- and third-lines. The pembrolizumab strategy is evaluated with and without the assumption that there is a LTS subgroup. The LTS subgroup is assumed to be free from metNSCLC-related progression after treatment. Costs (2022 €), including drug costs, other direct medical costs, family costs, and healthcare costs in life years gained, are considered from first-line treatment to death. Effects are measured in quality-adjusted life years (QALYs). The incremental cost-effectiveness ratio (ICER) is assessed using an €80,000/QALY threshold. Threshold analyses are performed on the size and mortality rate of the LTS subgroup and on the price of pembrolizumab.
Results: QALYs per patient were 0.65 for chemotherapy, 1.24 for pembrolizumab without LTS, and 3.52 for pembrolizumab with LTS. Average costs per patient were €58,800 for chemotherapy, €154,600 for pembrolizumab without LTS, and €178,600 for pembrolizumab with LTS. Pembrolizumab without LTS was not cost-effective compared with chemotherapy (ICER €167,600/QALY), but pembrolizumab with LTS (30% of simulated population) was cost effective (ICER of €43,100/QALY). Threshold analyses showed that a LTS subgroup size of at least 10% or halving the price of pembrolizumab was needed for pembrolizumab to be cost-effective.
Conclusions: Pembrolizumab is a cost-effective first-line treatment for patients with metNSCLC and PD-L1 ≥ 50% in the Netherlands when at least 10% of patients are long-term survivors. Without long-term survivors, this treatment is not cost-effective. Therefore, it is crucial to consider long-term survivors in assessing the cost-effectiveness of immunotherapy in metNSCLC.
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


