Katharina Seuthe, Eva Gerwin, Parwis Rahmanian, Bernd W Böttiger, Deepak Borde, Jakob Labus
{"title":"Intraoperative Course of Left Ventricular Diastolic Strain in Surgical Valve Replacement for Severe Aortic Valve Stenosis.","authors":"Katharina Seuthe, Eva Gerwin, Parwis Rahmanian, Bernd W Böttiger, Deepak Borde, Jakob Labus","doi":"10.4103/aca.aca_246_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Assessment of LV diastolic dysfunction (LVDD) poses challenges due to the dynamic changes of loading conditions in the perioperative course. Diastolic strain-based measures showed to be less load dependent, but data in aortic valve replacement (AVR) surgery remains sparse to date. Therefore, we aimed to explore the feasibility to assess these measurements and to describe the intraoperative course in this patient population.</p><p><strong>Methods: </strong>Prospective observational study including 30 adult patients. Intraoperative transesophageal echocardiography (TEE) was performed after induction of anesthesia [T1], after termination of cardiopulmonary bypass [T2], and after sternal closure [T3]. TEE assessment included the evaluation of peak longitudinal strain rate during isovolumetric relaxation (SR-IVR), early (SR-E) and late (SR-A) LV filling, as well as of conventional echocardiographic measurements and LVDD grading algorithms.</p><p><strong>Results: </strong>Diastolic strain analysis was feasible in 27 (90%) AVR patients at all time points of assessment. LV diastolic strain improved significantly after AVR [T1 vs T3] as measured by SR-IVR (0.31 s-1 (IQR 0.22; 0.38) vs. 0.4 s-1 (IQR 0.33; 0.43); P = 0.01), SR-E (1.13 s-1 (IQR 0.89;1.28) vs. 1.35 s-1 (IQR 1.10;1.52); P = 0.035), and E/SR-IVR (2.2 m (IQR 1.7;2.8) vs. 1.6 m (IQR 1.3;2.2); P = 0.013). In contrast, conventional echocardiographic measurements and grading algorithms were not able to detect these changes in the same period.</p><p><strong>Conclusion: </strong>Assessment of LV diastolic strain was feasible in our group of selected AVR patients. LV relaxation and filling improved during the intraoperative course of AVR as measured by diastolic strain, while most conventional grading algorithms were not able to detect these alterations.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"28 3","pages":"264-272"},"PeriodicalIF":1.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12324755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_246_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Assessment of LV diastolic dysfunction (LVDD) poses challenges due to the dynamic changes of loading conditions in the perioperative course. Diastolic strain-based measures showed to be less load dependent, but data in aortic valve replacement (AVR) surgery remains sparse to date. Therefore, we aimed to explore the feasibility to assess these measurements and to describe the intraoperative course in this patient population.
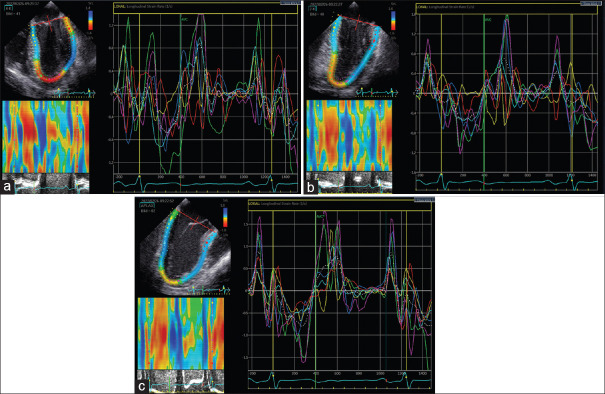
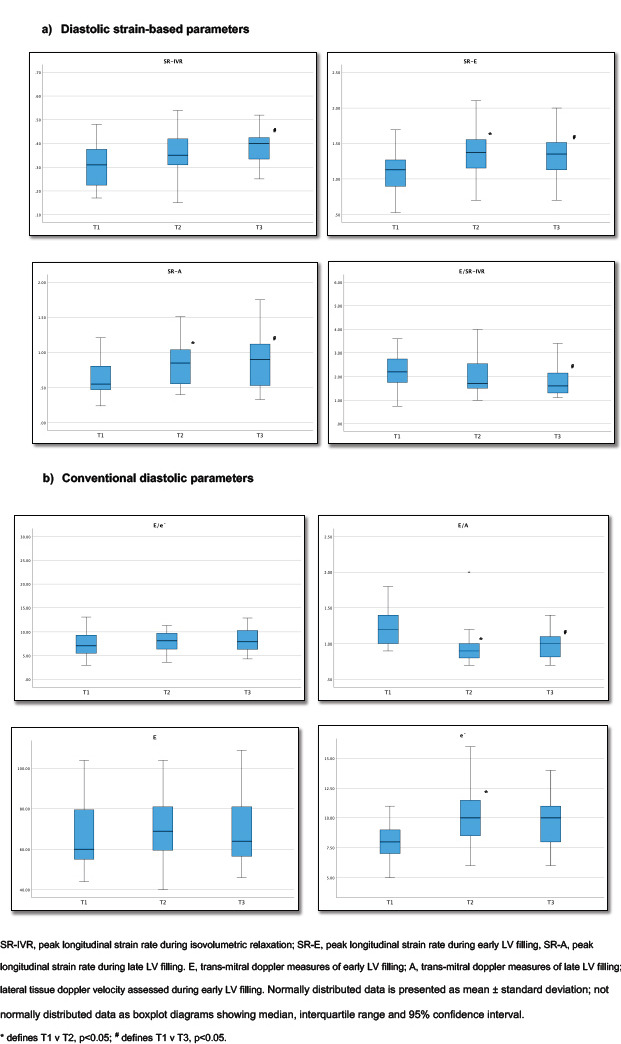
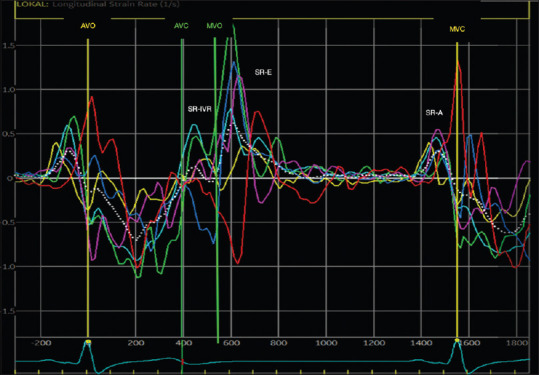
Methods: Prospective observational study including 30 adult patients. Intraoperative transesophageal echocardiography (TEE) was performed after induction of anesthesia [T1], after termination of cardiopulmonary bypass [T2], and after sternal closure [T3]. TEE assessment included the evaluation of peak longitudinal strain rate during isovolumetric relaxation (SR-IVR), early (SR-E) and late (SR-A) LV filling, as well as of conventional echocardiographic measurements and LVDD grading algorithms.
Results: Diastolic strain analysis was feasible in 27 (90%) AVR patients at all time points of assessment. LV diastolic strain improved significantly after AVR [T1 vs T3] as measured by SR-IVR (0.31 s-1 (IQR 0.22; 0.38) vs. 0.4 s-1 (IQR 0.33; 0.43); P = 0.01), SR-E (1.13 s-1 (IQR 0.89;1.28) vs. 1.35 s-1 (IQR 1.10;1.52); P = 0.035), and E/SR-IVR (2.2 m (IQR 1.7;2.8) vs. 1.6 m (IQR 1.3;2.2); P = 0.013). In contrast, conventional echocardiographic measurements and grading algorithms were not able to detect these changes in the same period.
Conclusion: Assessment of LV diastolic strain was feasible in our group of selected AVR patients. LV relaxation and filling improved during the intraoperative course of AVR as measured by diastolic strain, while most conventional grading algorithms were not able to detect these alterations.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


