[Clinical study on intravenous human immunoglobulin (pH4) for hypogammaglobulinemia and infection risk following CD20 monoclonal antibody therapy in patients with B-cell non-Hodgkin lymphoma].
{"title":"[Clinical study on intravenous human immunoglobulin (pH4) for hypogammaglobulinemia and infection risk following CD20 monoclonal antibody therapy in patients with B-cell non-Hodgkin lymphoma].","authors":"X K Li, Y F Shen, D P Wu, Y Xu","doi":"10.3760/cma.j.cn121090-20240918-00353","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> To observe the effect of intravenous human immunoglobulin (pH4) (IVIg) on total immunoglobulin (Ig) levels in patients with B-cell non-Hodgkin lymphoma (NHL) and to evaluate its clinical efficacy in ameliorating hypogammaglobulinemia following CD20 monoclonal antibody therapy. <b>Methods:</b> Clinical data of 98 patients with B-cell NHL who developed hypogammaglobulinemia after CD20 monoclonal antibody therapy and were hospitalized in the Department of Hematology, The First Affiliated Hospital of Soochow University, from January 2018 to June 2022, were retrospectively analyzed. Patients were divided into the IVIg group (<i>n</i>=70) and the conventional treatment group (<i>n</i>=28). To exclude the interference of plasma transfusion on total Ig levels, statistical analysis was performed on the IVIg group without plasma transfusion (<i>n</i>=53) and the conventional treatment group (<i>n</i>=25). The therapeutic efficacy of IVIg was analyzed by observing its effect on elevating total Ig levels and the duration of this effect. The infection control efficacy of IVIg was assessed by comparing other blood biochemical parameters. The safety of IVIg in clinical application was also evaluated. <b>Results:</b> In the IVIg group, the mean total Ig level within 1-3 days after IVIg treatment was (20.67±4.17) g/L, significantly higher than the pre-treatment level of (17.16±1.76) g/L (<i>P</i><0.001). In 22 patients from the IVIg group, total Ig levels at 1-7 days, 8-14 days, and 15-30 days post-treatment were all significantly different compared to pre-treatment levels (all <i>P</i><0.001). In the conventional treatment group, the mean total Ig level within 1-3 days after hospitalization showed no significant difference compared to the level at admission [ (18.12±1.84) g/L <i>vs</i> (18.43±1.79) g/L, <i>P</i>>0.05]. The proportion of patients in the IVIg group whose total Ig level reached 20 g/L within 1-3 days post-IVIg treatment was significantly higher than that in the conventional treatment group within 1-3 days after admission (57.69% <i>vs</i> 0, <i>P</i><0.001). In 12 patients from the IVIg group with baseline neutrophil levels below normal, neutrophil levels at 1-3 days, 4-7 days, and 8-14 days post-treatment were significantly increased compared to pre-treatment levels (all <i>P</i><0.05). The proportion of patients with new-onset infections post-treatment was lower in the IVIg group (22.64%, 12/53) than in the conventional treatment group (36.00%, 9/25), although the difference was not statistically significant (<i>P</i>>0.05). Among 70 patients in the IVIg group, 8 patients experienced grade 1-2 adverse reactions, including nausea and vomiting in 5 patients, rash in 2 patients, and muscle/joint pain in 1 patient. No grade 3 or higher adverse reactions were observed. <b>Conclusion:</b> IVIg increased Ig and neutrophil levels in patients with B-cell NHL after CD20 monoclonal antibody therapy and may play a role in controlling new-onset infections. IVIg is effective and safe for treating hypogammaglobulinemia secondary to CD20 monoclonal antibody therapy in patients with B-cell NHL.</p>","PeriodicalId":24016,"journal":{"name":"Zhonghua xue ye xue za zhi = Zhonghua xueyexue zazhi","volume":"46 5","pages":"425-430"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12268296/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Zhonghua xue ye xue za zhi = Zhonghua xueyexue zazhi","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3760/cma.j.cn121090-20240918-00353","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
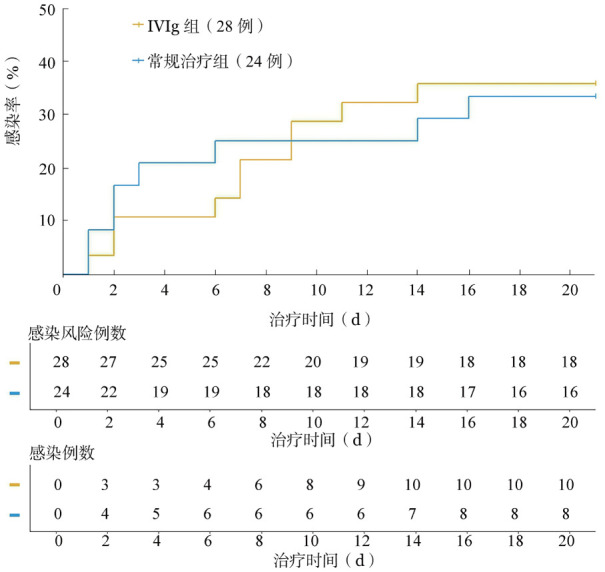
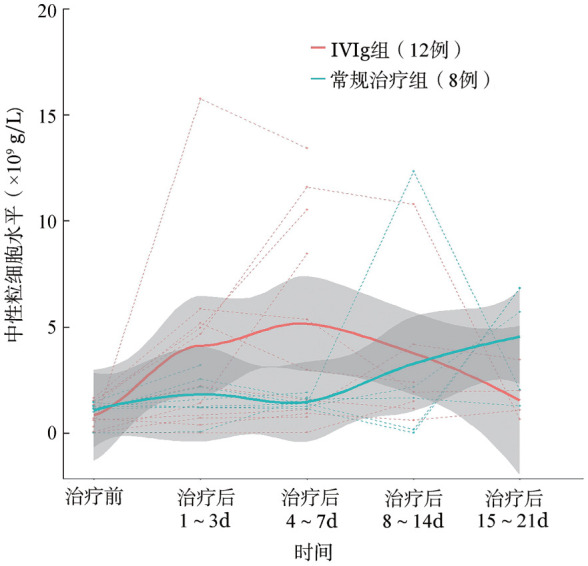
Objective: To observe the effect of intravenous human immunoglobulin (pH4) (IVIg) on total immunoglobulin (Ig) levels in patients with B-cell non-Hodgkin lymphoma (NHL) and to evaluate its clinical efficacy in ameliorating hypogammaglobulinemia following CD20 monoclonal antibody therapy. Methods: Clinical data of 98 patients with B-cell NHL who developed hypogammaglobulinemia after CD20 monoclonal antibody therapy and were hospitalized in the Department of Hematology, The First Affiliated Hospital of Soochow University, from January 2018 to June 2022, were retrospectively analyzed. Patients were divided into the IVIg group (n=70) and the conventional treatment group (n=28). To exclude the interference of plasma transfusion on total Ig levels, statistical analysis was performed on the IVIg group without plasma transfusion (n=53) and the conventional treatment group (n=25). The therapeutic efficacy of IVIg was analyzed by observing its effect on elevating total Ig levels and the duration of this effect. The infection control efficacy of IVIg was assessed by comparing other blood biochemical parameters. The safety of IVIg in clinical application was also evaluated. Results: In the IVIg group, the mean total Ig level within 1-3 days after IVIg treatment was (20.67±4.17) g/L, significantly higher than the pre-treatment level of (17.16±1.76) g/L (P<0.001). In 22 patients from the IVIg group, total Ig levels at 1-7 days, 8-14 days, and 15-30 days post-treatment were all significantly different compared to pre-treatment levels (all P<0.001). In the conventional treatment group, the mean total Ig level within 1-3 days after hospitalization showed no significant difference compared to the level at admission [ (18.12±1.84) g/L vs (18.43±1.79) g/L, P>0.05]. The proportion of patients in the IVIg group whose total Ig level reached 20 g/L within 1-3 days post-IVIg treatment was significantly higher than that in the conventional treatment group within 1-3 days after admission (57.69% vs 0, P<0.001). In 12 patients from the IVIg group with baseline neutrophil levels below normal, neutrophil levels at 1-3 days, 4-7 days, and 8-14 days post-treatment were significantly increased compared to pre-treatment levels (all P<0.05). The proportion of patients with new-onset infections post-treatment was lower in the IVIg group (22.64%, 12/53) than in the conventional treatment group (36.00%, 9/25), although the difference was not statistically significant (P>0.05). Among 70 patients in the IVIg group, 8 patients experienced grade 1-2 adverse reactions, including nausea and vomiting in 5 patients, rash in 2 patients, and muscle/joint pain in 1 patient. No grade 3 or higher adverse reactions were observed. Conclusion: IVIg increased Ig and neutrophil levels in patients with B-cell NHL after CD20 monoclonal antibody therapy and may play a role in controlling new-onset infections. IVIg is effective and safe for treating hypogammaglobulinemia secondary to CD20 monoclonal antibody therapy in patients with B-cell NHL.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


