Llucia Coll, Deborah Pareto, Francisco Aparicio-Serrano, Susana Otero-Romero, Alvaro Cobo-Calvo, Evy Reinders, Manel Alberich, María Jesús Arévalo, Georgina Arrambide, Cristina Auger, Joaquín Castilló, Manuel Comabella, Ingrid Galán, Luciana Midaglia, Carlos Nos, Frederik Novak, Arnau Oliver, Jordi Río, Breogán Rodríguez-Acevedo, Jaume Sastre-Garriga, Ángela Vidal-Jordana, Ana Zabalza, Xavier Montalban, Àlex Rovira, Mar Tintoré, Xavier Lladó, Carmen Tur
{"title":"Deep learning to predict progression independent of relapse activity at a first demyelinating event.","authors":"Llucia Coll, Deborah Pareto, Francisco Aparicio-Serrano, Susana Otero-Romero, Alvaro Cobo-Calvo, Evy Reinders, Manel Alberich, María Jesús Arévalo, Georgina Arrambide, Cristina Auger, Joaquín Castilló, Manuel Comabella, Ingrid Galán, Luciana Midaglia, Carlos Nos, Frederik Novak, Arnau Oliver, Jordi Río, Breogán Rodríguez-Acevedo, Jaume Sastre-Garriga, Ángela Vidal-Jordana, Ana Zabalza, Xavier Montalban, Àlex Rovira, Mar Tintoré, Xavier Lladó, Carmen Tur","doi":"10.1093/braincomms/fcaf243","DOIUrl":null,"url":null,"abstract":"<p><p>Progression independent of relapse activity is the main cause of irreversible disability in multiple sclerosis and is strongly associated with older age at symptom onset. Early and accurate prediction, at symptom onset, of which patients are at highest risk of progression independent of relapses, is an unmet need. This study aimed to develop a deep learning survival model using only routine MRI acquired at the first demyelinating attack to predict the risk of progression independent of relapses, and assess its ability to improve classical age-adjusted predictions. We analysed a prospective cohort of patients under 50, clinically assessed within three months of symptom onset, with available MRI (T1- and T2-Fluid-Attenuated Inversion Recovery sequences). An independent early multiple sclerosis cohort (≤1 year from symptom onset) from the Multiple Sclerosis Partners Advancing Technology and Health Solutions database (<i>N</i> = 32) was used for external validation. Patients were assessed for progression independent of relapse activity, defined as a 6-month confirmed increase in the Expanded Disability Status Scale without relapses. Our deep learning model used EfficientNet to estimate the cumulative probability of progression independent of relapses at 1-year intervals. We employed 5-fold cross-validation for model training and testing, assessing performance with the time-dependent concordance index. We also investigated the optimal cumulative probability threshold for binary risk stratification. The model's ability to improve a classical Cox regression model was evaluated. Additionally, we identified brain regions most relevant to deep learning-based progression independent of relapse activity predictions using an interpretability algorithm. A total of 259 patients were evaluated, 58 (22%) of whom experienced at least one event of progression independent of relapse activity over a median follow-up of 4.2 years. The deep learning model demonstrated high performance (time-dependent concordance index = 0.72) with an accuracy of 78% in the original cohort and 72% in the external cohort for predicting the risk of progression independent of relapse activity. Incorporating the deep learning-derived cumulative probability of progression independent of relapses significantly improved an age-adjusted Cox regression model, raising Harrell's C index from 0.62 to 0.74. Interpretability revealed the frontoparietal cortex as a key region in predicting progression independent of relapse activity. In conclusion, our deep learning survival model, based on routine MRI at the first demyelinating attack, can accurately identify patients at high risk of progression independent of relapses and may serve as a valuable tool in clinical practice.</p>","PeriodicalId":93915,"journal":{"name":"Brain communications","volume":"7 4","pages":"fcaf243"},"PeriodicalIF":4.5000,"publicationDate":"2025-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226453/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/braincomms/fcaf243","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
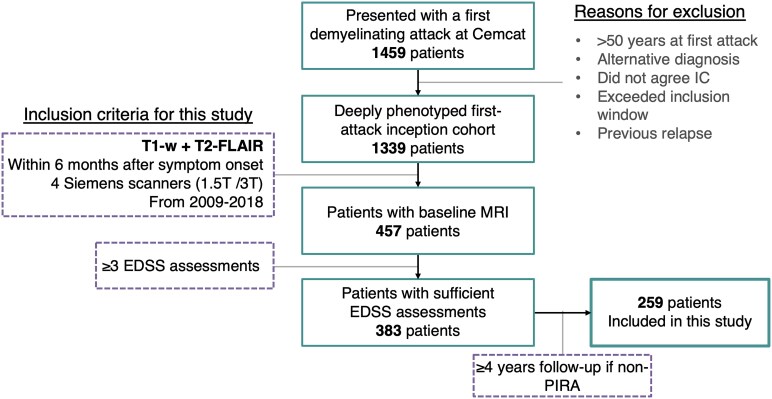
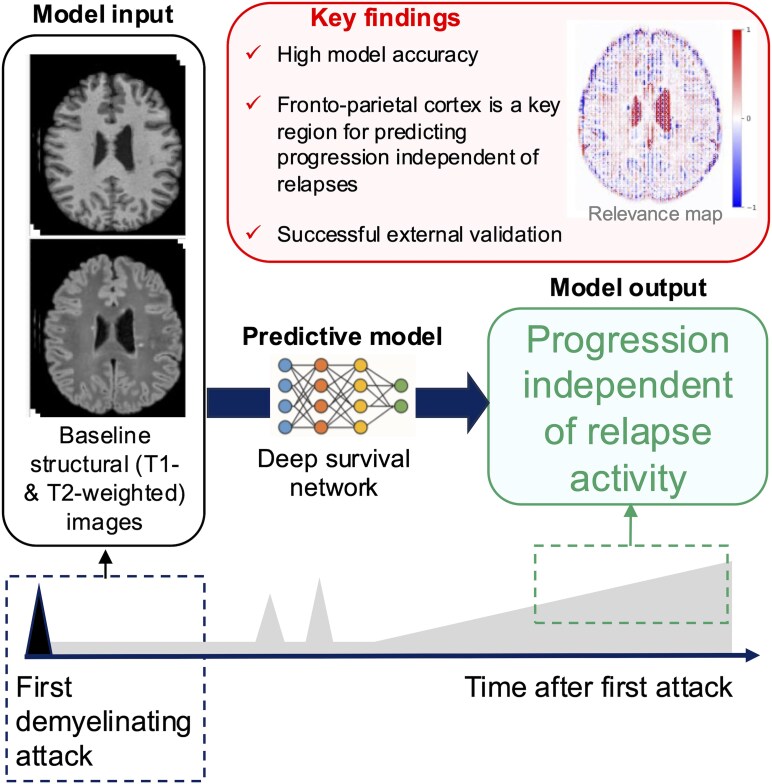
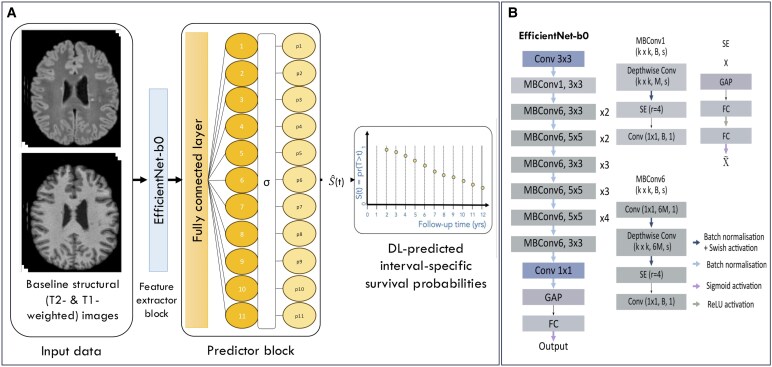
Progression independent of relapse activity is the main cause of irreversible disability in multiple sclerosis and is strongly associated with older age at symptom onset. Early and accurate prediction, at symptom onset, of which patients are at highest risk of progression independent of relapses, is an unmet need. This study aimed to develop a deep learning survival model using only routine MRI acquired at the first demyelinating attack to predict the risk of progression independent of relapses, and assess its ability to improve classical age-adjusted predictions. We analysed a prospective cohort of patients under 50, clinically assessed within three months of symptom onset, with available MRI (T1- and T2-Fluid-Attenuated Inversion Recovery sequences). An independent early multiple sclerosis cohort (≤1 year from symptom onset) from the Multiple Sclerosis Partners Advancing Technology and Health Solutions database (N = 32) was used for external validation. Patients were assessed for progression independent of relapse activity, defined as a 6-month confirmed increase in the Expanded Disability Status Scale without relapses. Our deep learning model used EfficientNet to estimate the cumulative probability of progression independent of relapses at 1-year intervals. We employed 5-fold cross-validation for model training and testing, assessing performance with the time-dependent concordance index. We also investigated the optimal cumulative probability threshold for binary risk stratification. The model's ability to improve a classical Cox regression model was evaluated. Additionally, we identified brain regions most relevant to deep learning-based progression independent of relapse activity predictions using an interpretability algorithm. A total of 259 patients were evaluated, 58 (22%) of whom experienced at least one event of progression independent of relapse activity over a median follow-up of 4.2 years. The deep learning model demonstrated high performance (time-dependent concordance index = 0.72) with an accuracy of 78% in the original cohort and 72% in the external cohort for predicting the risk of progression independent of relapse activity. Incorporating the deep learning-derived cumulative probability of progression independent of relapses significantly improved an age-adjusted Cox regression model, raising Harrell's C index from 0.62 to 0.74. Interpretability revealed the frontoparietal cortex as a key region in predicting progression independent of relapse activity. In conclusion, our deep learning survival model, based on routine MRI at the first demyelinating attack, can accurately identify patients at high risk of progression independent of relapses and may serve as a valuable tool in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


