Clinical outcomes of high-risk patients with polycythemia vera after suboptimal response to first-line therapy who switched to ruxolitinib versus nonswitchers: results from the PV-Switch study.
Steffen Koschmieder, Clemens Schulte, Eyck von der Heyde, Lambert Busque, Françoise Boyer-Perrard, Timothy Devos, Francesco Passamonti, Wendy Y Cheng, Mu Cheng, Marja Nuortti, Volker Baum, Claire Harrison
{"title":"Clinical outcomes of high-risk patients with polycythemia vera after suboptimal response to first-line therapy who switched to ruxolitinib versus nonswitchers: results from the PV-Switch study.","authors":"Steffen Koschmieder, Clemens Schulte, Eyck von der Heyde, Lambert Busque, Françoise Boyer-Perrard, Timothy Devos, Francesco Passamonti, Wendy Y Cheng, Mu Cheng, Marja Nuortti, Volker Baum, Claire Harrison","doi":"10.1177/20406207251342199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cytoreductive therapies have been the standard treatment for patients with high-risk polycythemia vera (PV) for decades. However, approximately 24% of patients treated with hydroxyurea will eventually develop resistance or intolerance to hydroxyurea and need second-line (2L) therapy.</p><p><strong>Objective: </strong>This study compared clinical outcomes of patients with high-risk PV who switched to ruxolitinib as 2L therapy (switchers) versus those who continued first-line (1L) therapy (nonswitchers) after suboptimal response.</p><p><strong>Design: </strong>This was a retrospective, multicenter, noninterventional study.</p><p><strong>Methods: </strong>The primary outcome was event-free survival (EFS), defined as the time between the index date and the earliest event of thrombosis, major bleeding, disease progression, or death. Key secondary outcomes included overall survival (OS), time to and rate of disease progression, rate of thrombosis, and change in spleen size.</p><p><strong>Results: </strong>Overall, 225 patients were included (switchers: 69; nonswitchers: 156). At baseline, >50% of switchers had a prior history of thrombosis (<i>p</i> = 0.006) and PV-related symptoms (<i>p</i> = 0.037) versus nonswitchers. Switchers had a numerically greater reduction in spleen size at 3 years than nonswitchers (-14.4% vs +15.9%; <i>p</i> = 0.107). Compared with nonswitchers, switchers were more likely to experience persistence or presence of new PV-related symptoms as suboptimal response before switching to ruxolitinib (<i>p</i> < 0.001). A greater proportion of nonswitchers required ⩾3 phlebotomies to maintain hematocrit <45% within 1 year (<i>p</i> < 0.001). No significant differences were observed between switchers and nonswitchers in terms of EFS, OS, time to disease progression, and rate of thrombosis. However, switchers had a significantly higher rate of disease progression to myelofibrosis than nonswitchers (<i>p</i> = 0.016).</p><p><strong>Conclusion: </strong>These data demonstrate the heterogeneity in patient characteristics and type of suboptimal responses between switchers and nonswitchers. The results suggest that patients who switched to ruxolitinib had more severe disease or rapid disease progression and that ruxolitinib may provide some clinical benefit in terms of spleen size reduction and hematocrit control.</p>","PeriodicalId":23048,"journal":{"name":"Therapeutic Advances in Hematology","volume":"16 ","pages":"20406207251342199"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227902/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Hematology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20406207251342199","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cytoreductive therapies have been the standard treatment for patients with high-risk polycythemia vera (PV) for decades. However, approximately 24% of patients treated with hydroxyurea will eventually develop resistance or intolerance to hydroxyurea and need second-line (2L) therapy.
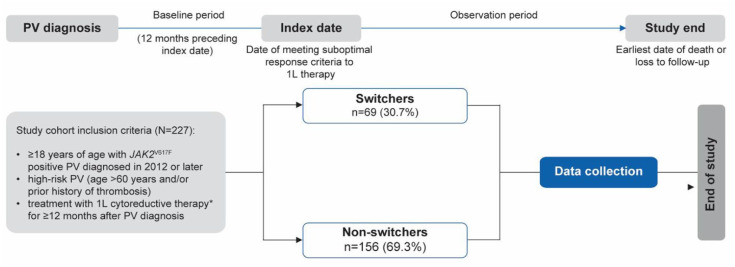
Objective: This study compared clinical outcomes of patients with high-risk PV who switched to ruxolitinib as 2L therapy (switchers) versus those who continued first-line (1L) therapy (nonswitchers) after suboptimal response.
Design: This was a retrospective, multicenter, noninterventional study.
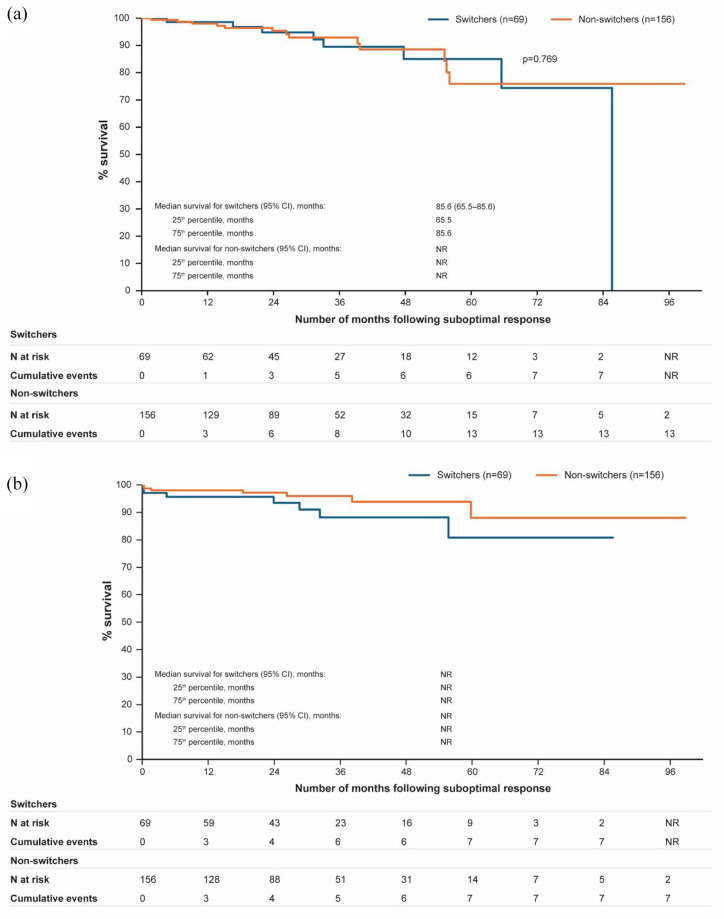
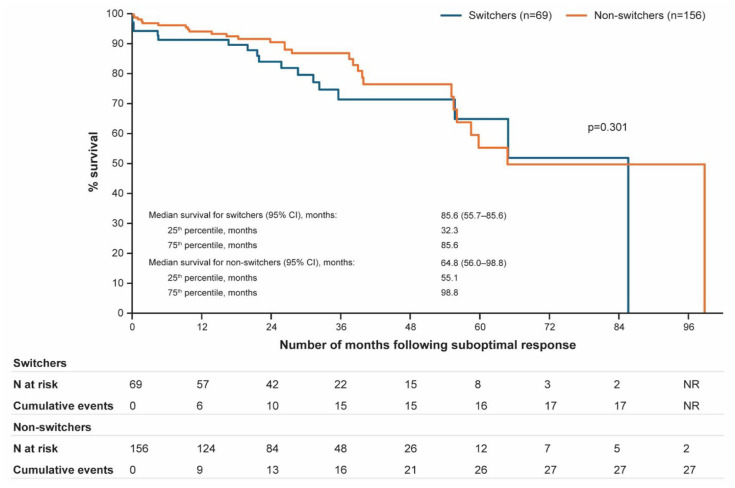
Methods: The primary outcome was event-free survival (EFS), defined as the time between the index date and the earliest event of thrombosis, major bleeding, disease progression, or death. Key secondary outcomes included overall survival (OS), time to and rate of disease progression, rate of thrombosis, and change in spleen size.
Results: Overall, 225 patients were included (switchers: 69; nonswitchers: 156). At baseline, >50% of switchers had a prior history of thrombosis (p = 0.006) and PV-related symptoms (p = 0.037) versus nonswitchers. Switchers had a numerically greater reduction in spleen size at 3 years than nonswitchers (-14.4% vs +15.9%; p = 0.107). Compared with nonswitchers, switchers were more likely to experience persistence or presence of new PV-related symptoms as suboptimal response before switching to ruxolitinib (p < 0.001). A greater proportion of nonswitchers required ⩾3 phlebotomies to maintain hematocrit <45% within 1 year (p < 0.001). No significant differences were observed between switchers and nonswitchers in terms of EFS, OS, time to disease progression, and rate of thrombosis. However, switchers had a significantly higher rate of disease progression to myelofibrosis than nonswitchers (p = 0.016).
Conclusion: These data demonstrate the heterogeneity in patient characteristics and type of suboptimal responses between switchers and nonswitchers. The results suggest that patients who switched to ruxolitinib had more severe disease or rapid disease progression and that ruxolitinib may provide some clinical benefit in terms of spleen size reduction and hematocrit control.
期刊介绍:
Therapeutic Advances in Hematology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of hematology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in hematology, providing a forum in print and online for publishing the highest quality articles in this area.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


