Venous thromboembolism chemoprophylaxis is not supported following elective spine surgery: a systematic review and meta-analysis of randomized controlled trials.
Aditya Muralidharan, Davin C Gong, Anthony N Baumann, Joshua D Piche, Kempland C Walley, Osama N Kashlan, Rakesh D Patel, Ilyas S Aleem
{"title":"Venous thromboembolism chemoprophylaxis is not supported following elective spine surgery: a systematic review and meta-analysis of randomized controlled trials.","authors":"Aditya Muralidharan, Davin C Gong, Anthony N Baumann, Joshua D Piche, Kempland C Walley, Osama N Kashlan, Rakesh D Patel, Ilyas S Aleem","doi":"10.21037/jss-24-162","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pharmacologic venous thromboembolism (VTE) prophylaxis following spine surgery is not standardized. This study aims to compare the rates of VTE between patients receiving chemoprophylaxis <i>vs.</i> no chemoprophylaxis following elective spine surgery.</p><p><strong>Methods: </strong>A comprehensive investigation of searchable electronic databases was performed to capture randomized controlled trials (RCTs) comparing VTE chemoprophylaxis with no chemoprophylaxis after elective spine surgery. Two authors examined the eligibility, risk of bias and quality of studies using the Grades of Recommendation Assessment, Development and Evaluation (GRADE) criteria. Meta-analyses were conducted for risk of developing VTE, including deep vein thrombosis (DVT) and pulmonary embolism (PE), significant bleeding, and epidural hematoma.</p><p><strong>Results: </strong>After appraising 2,666 articles, eight RCTs were ultimately included in the analysis. These trials involved 1,509 patients, with 1,151 receiving VTE chemoprophylaxis and 358 not receiving it. No significant differences were found between the groups in the incidence of VTE [risk ratio (RR): 1.01; 95% confidence interval (CI): 0.97, 1.05; P=0.68] or DVT (RR: 1.03; 95% CI: 0.99, 1.06; P=0.11). Additionally, there were no significant differences in the risk of severe bleeding (RR: 1.01; 95% CI: 0.97, 1.05; P=0.59), significant bleeding (RR: 1.01; 95% CI: 0.97, 1.04; P=0.75), PE (RR: 1.00; 95% CI: 0.96, 1.03; P=0.81), or epidural hematoma (RR: 1.00; 95% CI: 0.97, 1.03; P>0.99) between the groups.</p><p><strong>Conclusions: </strong>This systematic review and meta-analysis did not find a statistically significant difference in the efficacy of routine use of VTE chemoprophylaxis following elective spine surgery with moderate-quality evidence. Future well-designed randomized trials with adequate power are still needed to assess the safety and efficacy of VTE chemoprophylaxis, especially considering the variability of surgical techniques in elective spine surgery.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"11 2","pages":"242-255"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226186/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-162","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pharmacologic venous thromboembolism (VTE) prophylaxis following spine surgery is not standardized. This study aims to compare the rates of VTE between patients receiving chemoprophylaxis vs. no chemoprophylaxis following elective spine surgery.
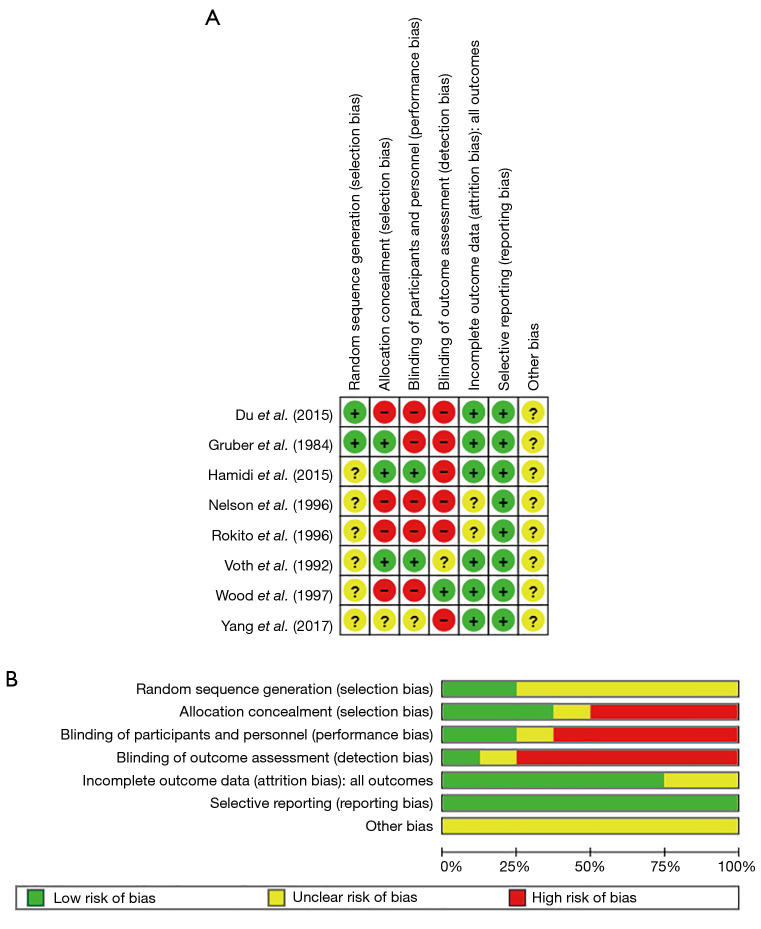
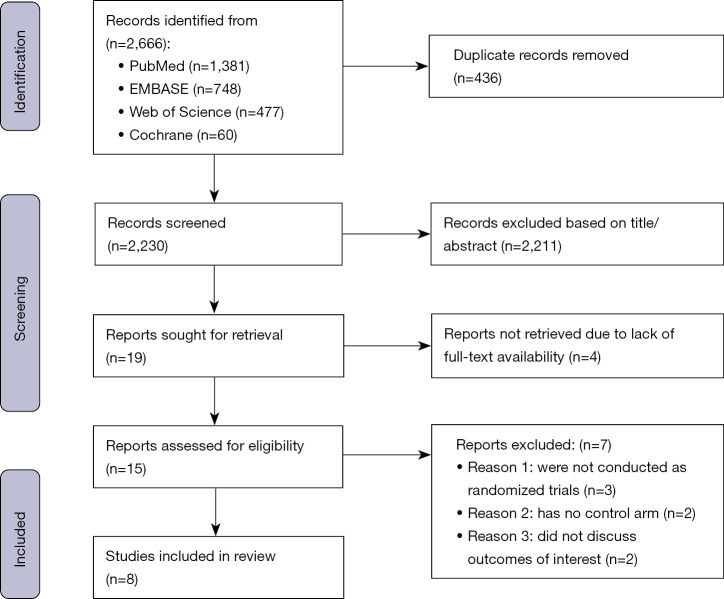
Methods: A comprehensive investigation of searchable electronic databases was performed to capture randomized controlled trials (RCTs) comparing VTE chemoprophylaxis with no chemoprophylaxis after elective spine surgery. Two authors examined the eligibility, risk of bias and quality of studies using the Grades of Recommendation Assessment, Development and Evaluation (GRADE) criteria. Meta-analyses were conducted for risk of developing VTE, including deep vein thrombosis (DVT) and pulmonary embolism (PE), significant bleeding, and epidural hematoma.
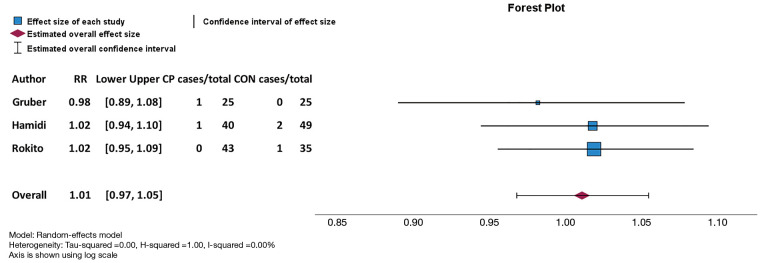
Results: After appraising 2,666 articles, eight RCTs were ultimately included in the analysis. These trials involved 1,509 patients, with 1,151 receiving VTE chemoprophylaxis and 358 not receiving it. No significant differences were found between the groups in the incidence of VTE [risk ratio (RR): 1.01; 95% confidence interval (CI): 0.97, 1.05; P=0.68] or DVT (RR: 1.03; 95% CI: 0.99, 1.06; P=0.11). Additionally, there were no significant differences in the risk of severe bleeding (RR: 1.01; 95% CI: 0.97, 1.05; P=0.59), significant bleeding (RR: 1.01; 95% CI: 0.97, 1.04; P=0.75), PE (RR: 1.00; 95% CI: 0.96, 1.03; P=0.81), or epidural hematoma (RR: 1.00; 95% CI: 0.97, 1.03; P>0.99) between the groups.
Conclusions: This systematic review and meta-analysis did not find a statistically significant difference in the efficacy of routine use of VTE chemoprophylaxis following elective spine surgery with moderate-quality evidence. Future well-designed randomized trials with adequate power are still needed to assess the safety and efficacy of VTE chemoprophylaxis, especially considering the variability of surgical techniques in elective spine surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


