Contemporaneously diagnosed lumbosacral spinal subdural hematoma and cranial subdural hematoma with cerebral contusions following isolated head trauma: a case report and review of the literature.
Ibrahim Nabhan, Nova Kristine de Los Reyes-Nabhan, Farschad Tabesch, Andrei Slavici, Michael Rauschmann
{"title":"Contemporaneously diagnosed lumbosacral spinal subdural hematoma and cranial subdural hematoma with cerebral contusions following isolated head trauma: a case report and review of the literature.","authors":"Ibrahim Nabhan, Nova Kristine de Los Reyes-Nabhan, Farschad Tabesch, Andrei Slavici, Michael Rauschmann","doi":"10.21037/jss-24-120","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Concurrent spinal subdural hematoma (SSDH) and cranial subdural hematoma (CSDH) have been sporadically reported. However, concurrent SSDH and CSDH with intracerebral hemorrhage (ICH) is extremely rare.</p><p><strong>Case description: </strong>A previously healthy 19-year-old man presented with symptoms of intracranial hypertension and back pain with radiculopathy without focal neurologic deficits. Craniospinal magnetic resonance imaging (MRI) detected bilateral CSDHs, cerebral contusions, and lumbosacral, anterior SSDH simultaneously, 1 week after isolated head trauma and unremarkable cranial computed tomography (CT). A positive \"inverted Mercedes-Benz sign\" in axial T1 and T2 sequences confirmed the diagnosis. We report the first case of contemporaneously diagnosed SSDH and CSDH with cerebral contusions following head trauma without spinal trauma, whereby all pathologies were managed conservatively. Furthermore, we performed a review of pertinent literature available in PubMed. Twelve cases with contemporaneous diagnosis of CSDH and SSDH within a narrow diagnostic timeframe of ≤48 hours were published since 2005. All but one was male with a mean age of 41.5 years (range, 11-70 years). Fifty percent reported cranial trauma. Nine cases (66.7%) had headaches, and 10 patients (83.3%) reported radiculopathy. Nine patients (66.7%) reported cranial and spinal symptoms. All 5 patients (41.7%) treated conservatively for both pathologies showed complete clinical and radiological resolution at follow-up.</p><p><strong>Conclusions: </strong>Our case exemplifies the effectiveness and favorable outcome of conservative management in neurologically intact SSDH with radiculopathy. Twelve cases of concurrent CSDH and SSDH diagnosed within a timeframe of ≤48 hours were included in the review. We discuss three theories proposed in the literature explaining pathomechanisms of traumatic SSDH and its plausible causational relationship with CSDH. SSDH can occur with all types of intracranial hemorrhage. Lower thresholds for ordering cranial imaging upon evidence of traumatic SSDH could allow detection of occult CSDH. Spinal imaging should be conducted in head trauma patients with spinal symptoms regardless of neurologic status to exclude possible SSDH. Older patients with higher risk of rebleeding often receive surgical evacuation of CSDHs. Extensive SSDHs with neurologic deficits are surgically evacuated to relieve neural compression. Conservative management of CSDH and/or SSDH is reasonable in younger patients without deficits. Regardless of management strategies, prognosis is generally good with very low complication rates.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"11 2","pages":"378-386"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226178/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Concurrent spinal subdural hematoma (SSDH) and cranial subdural hematoma (CSDH) have been sporadically reported. However, concurrent SSDH and CSDH with intracerebral hemorrhage (ICH) is extremely rare.
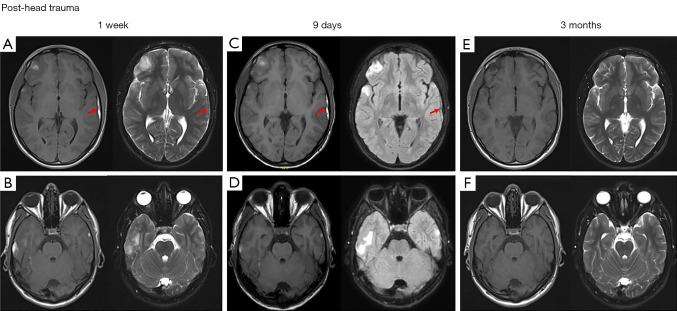
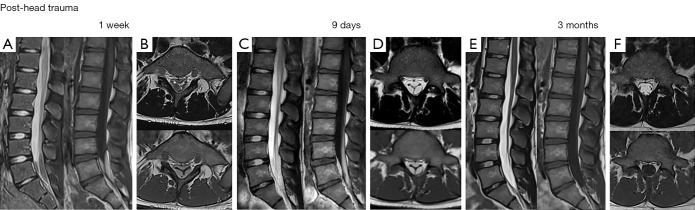
Case description: A previously healthy 19-year-old man presented with symptoms of intracranial hypertension and back pain with radiculopathy without focal neurologic deficits. Craniospinal magnetic resonance imaging (MRI) detected bilateral CSDHs, cerebral contusions, and lumbosacral, anterior SSDH simultaneously, 1 week after isolated head trauma and unremarkable cranial computed tomography (CT). A positive "inverted Mercedes-Benz sign" in axial T1 and T2 sequences confirmed the diagnosis. We report the first case of contemporaneously diagnosed SSDH and CSDH with cerebral contusions following head trauma without spinal trauma, whereby all pathologies were managed conservatively. Furthermore, we performed a review of pertinent literature available in PubMed. Twelve cases with contemporaneous diagnosis of CSDH and SSDH within a narrow diagnostic timeframe of ≤48 hours were published since 2005. All but one was male with a mean age of 41.5 years (range, 11-70 years). Fifty percent reported cranial trauma. Nine cases (66.7%) had headaches, and 10 patients (83.3%) reported radiculopathy. Nine patients (66.7%) reported cranial and spinal symptoms. All 5 patients (41.7%) treated conservatively for both pathologies showed complete clinical and radiological resolution at follow-up.
Conclusions: Our case exemplifies the effectiveness and favorable outcome of conservative management in neurologically intact SSDH with radiculopathy. Twelve cases of concurrent CSDH and SSDH diagnosed within a timeframe of ≤48 hours were included in the review. We discuss three theories proposed in the literature explaining pathomechanisms of traumatic SSDH and its plausible causational relationship with CSDH. SSDH can occur with all types of intracranial hemorrhage. Lower thresholds for ordering cranial imaging upon evidence of traumatic SSDH could allow detection of occult CSDH. Spinal imaging should be conducted in head trauma patients with spinal symptoms regardless of neurologic status to exclude possible SSDH. Older patients with higher risk of rebleeding often receive surgical evacuation of CSDHs. Extensive SSDHs with neurologic deficits are surgically evacuated to relieve neural compression. Conservative management of CSDH and/or SSDH is reasonable in younger patients without deficits. Regardless of management strategies, prognosis is generally good with very low complication rates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


