Preferences for TB treatment and support delivery models among people living with TB in Eastern Cape, South Africa: a discrete choice experiment
Abstract
Introduction
South Africa has one of the highest incidence rates of notified tuberculosis (TB) in the world. Achieving TB control requires strengthening treatment and support services. The implementation of differentiated delivery models can be used to improve service quality and enhance retention in care. This study aimed to identify treatment and support delivery preferences among people on TB treatment, specifically examining gender differences, to inform the development of differentiated care models for improving engagement and retention in TB treatment services.
Methods
A binary, unlabelled, fractional factorial design discrete choice experiment (DCE) was used to investigate preferences for TB treatment adherence support and service delivery. Attributes included who provides the support, how and where support is delivered, medication collection location and frequency of clinic visits. The DCE was administered to individuals who were currently on or recently completed TB treatment, and to those at-risk for being lost-to-care. Data from 284 individuals for the DCE were collected from March to August 2022. Mixed effects logistic regression models were used as primary analysis tools. Latent class analysis (LCA) was used to explore heterogeneity in preference structures.
Results
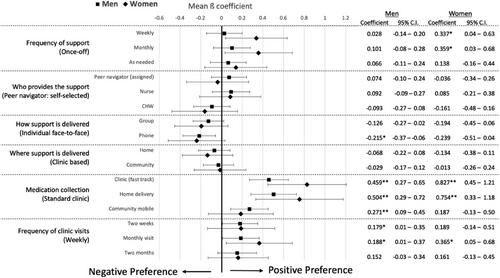
Compared to standard clinic-based treatment collection, participants preferred collecting their treatment from a mobile community-based location (ß = 0.231; 95% CI: 0.08–0.39), clinic-based fast-tracked pick-ups (ß = 0.539; 95% CI: 0.38–0.70) or home delivery (ß = 0.563; 95% CI: 0.37–0.75). Participants also significantly preferred support offered monthly compared to once-off (ß = 0.167; 95% CI: 0.01–0.32). Furthermore, participants preferred face-to-face support over group (ß = –0.142; 95% CI: –0.27 to –0.02) or phone-based (ß = –0.222; 95% CI: –0.36 to –0.09) support models. LCA revealed three classes with statistically similar preference structures; Class 1 (62%) preferred community-based treatment delivery and support services; Class 2 (28%) preferred clinic-based support and treatment delivery services; and Class 3 (10%), preferred self-selected peer navigator or nurse delivered, and group models of support and prioritised the location of medication pickups, with a preference for any model other than standard clinic collection.
Conclusions
Though preference structures did not differ by gender, respondents revealed strong preferences for differentiated service delivery models. Future TB treatment and support interventions must include both clinic- and community-based models of care and support to ensure that those living with TB are provided the greatest access to TB treatment and support services.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


