{"title":"Perforated meckel's diverticulum misdiagnosed as a urinary tract infection in an 11-year-old adolescent: case report of a rare differential diagnosis.","authors":"Mohamed Ali, Hisham Hazem Warda, Ahmed Elghrieb","doi":"10.1186/s13037-025-00443-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Meckel's diverticulum, a congenital anomaly of the gastrointestinal tract, is often asymptomatic but can present with complications such as inflammation, perforation, or obstruction. Misdiagnosis is common owing to its varied presentations, particularly when symptoms mimic other conditions such as urinary tract infections (UTI).</p><p><strong>Case presentation: </strong>An 11-year-old boy presented with persistent suprapubic pain and dysuria for one week. Initial urine analysis revealed turbid urine with high numbers of red blood cells, leading to a diagnosis of urinary tract infection (UTI), and antibiotic treatment was initiated. However, the patient's symptoms persisted, with worsening clinical signs. A complete blood count revealed leukocytosis with neutrophilia, suggesting the need for further evaluation. A non contrast computed tomography (CT) scan revealed a thickened, blind-ended structure in the midline lower abdomen with gas, extensive fat stranding, and associated mesenteric lymphadenopathy, suggestive of perforated Meckel's diverticulum. The patient underwent laparoscopic exploration, which revealed an abscess caused by perforated Meckel's diverticulum adherent to the urinary bladder. Diverticulectomy and incidental appendectomy were performed via a stapling device. Pathology confirmed a perforation of Meckel's diverticulum with serofibrinous peritonitis and follicular appendicitis. The postoperative course was uneventful, with the patient resuming full oral intake by the fifth day and being discharged in stable condition.</p><p><strong>Conclusion: </strong>This case emphasizes how Meckel's diverticulum can mimic a urinary tract infection, especially in pediatric patients with overlapping symptoms like suprapubic pain and dysuria. The delayed diagnosis highlights the importance of reconsidering rare causes when symptoms persist. Timely imaging was crucial in guiding effective treatment.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"19 1","pages":"20"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231995/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-025-00443-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Meckel's diverticulum, a congenital anomaly of the gastrointestinal tract, is often asymptomatic but can present with complications such as inflammation, perforation, or obstruction. Misdiagnosis is common owing to its varied presentations, particularly when symptoms mimic other conditions such as urinary tract infections (UTI).
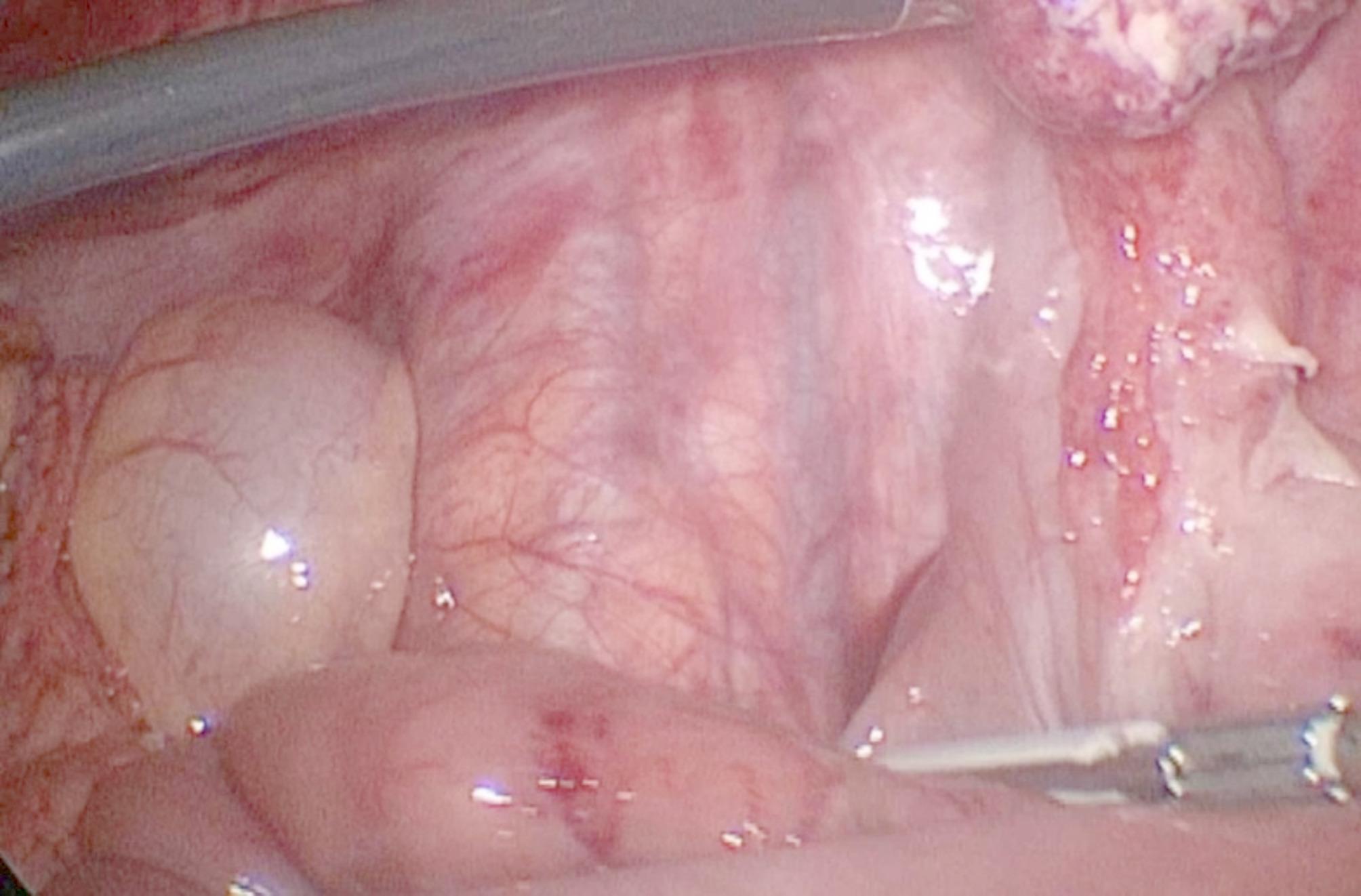
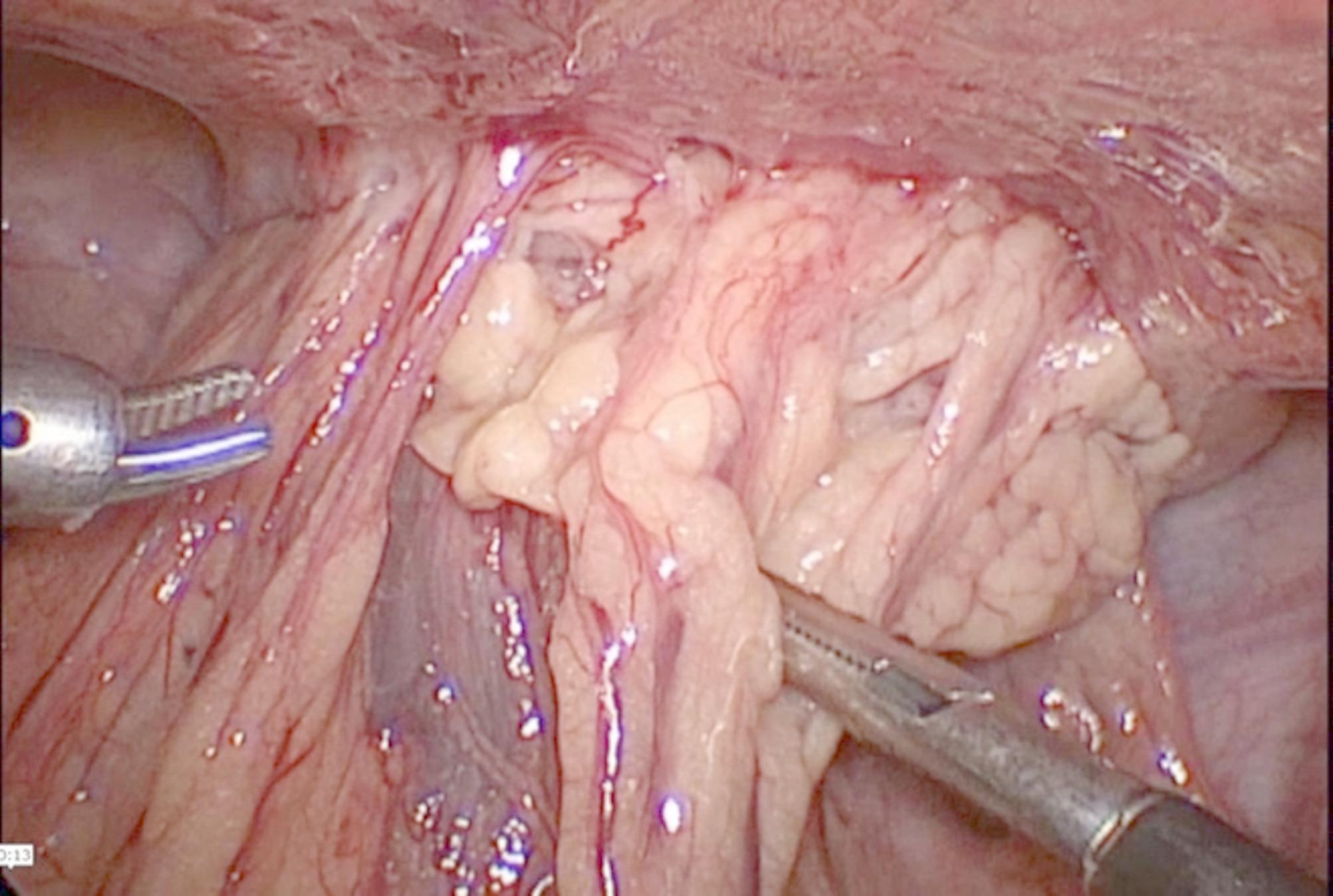
Case presentation: An 11-year-old boy presented with persistent suprapubic pain and dysuria for one week. Initial urine analysis revealed turbid urine with high numbers of red blood cells, leading to a diagnosis of urinary tract infection (UTI), and antibiotic treatment was initiated. However, the patient's symptoms persisted, with worsening clinical signs. A complete blood count revealed leukocytosis with neutrophilia, suggesting the need for further evaluation. A non contrast computed tomography (CT) scan revealed a thickened, blind-ended structure in the midline lower abdomen with gas, extensive fat stranding, and associated mesenteric lymphadenopathy, suggestive of perforated Meckel's diverticulum. The patient underwent laparoscopic exploration, which revealed an abscess caused by perforated Meckel's diverticulum adherent to the urinary bladder. Diverticulectomy and incidental appendectomy were performed via a stapling device. Pathology confirmed a perforation of Meckel's diverticulum with serofibrinous peritonitis and follicular appendicitis. The postoperative course was uneventful, with the patient resuming full oral intake by the fifth day and being discharged in stable condition.
Conclusion: This case emphasizes how Meckel's diverticulum can mimic a urinary tract infection, especially in pediatric patients with overlapping symptoms like suprapubic pain and dysuria. The delayed diagnosis highlights the importance of reconsidering rare causes when symptoms persist. Timely imaging was crucial in guiding effective treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


