Nicolas Polge, Camille Hego, Jules Grégory, Sophie Hamada, Anne Godier, Jean Charles Bijot, Axelle Dupont, Paer-Selim Abback, Caroline Jeantrelle, Emmanuel Weiss, Jean Denis Moyer
{"title":"Impact of severe splenic trauma and its management on the occurrence of infections in intensive care unit.","authors":"Nicolas Polge, Camille Hego, Jules Grégory, Sophie Hamada, Anne Godier, Jean Charles Bijot, Axelle Dupont, Paer-Selim Abback, Caroline Jeantrelle, Emmanuel Weiss, Jean Denis Moyer","doi":"10.1136/tsaco-2024-001704","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Severe trauma can be responsible for a major systemic inflammatory response followed by post-traumatic immunosuppression. Immune imbalance promotes infections and increases mortality. This risk could be further increased in case of impaired splenic immune function due to splenic trauma. The objective of this study was to evaluate whether severe splenic trauma increased infectious complications in trauma patients during intensive care unit (ICU) stay.</p><p><strong>Methods: </strong>This was an observational, bicentric, retrospective, case-control study including patients admitted for severe trauma from January 2011 to December 2020 in two level 1 trauma centers. Patients with American Association for the Surgery of Trauma (AAST) ≥III splenic trauma (case) were matched (1:3) with patients without splenic trauma (controls) according to age, sex, Injury Severity Score, initial Glasgow Coma Score, and Simplified Acute Physiology Score II. Demographic, trauma management, and infection data were collected. The primary endpoint was the incidence density of any infectious disease during ICU stay.</p><p><strong>Results: </strong>Among 7,304 severe trauma patients, 130 patients with AAST ≥III splenic trauma were included. 10 patients could not be matched with controls. 17 patients (14.1%) underwent splenectomy, 56 patients (46.7%) had non-operative management with arterioembolization, and 47 (39.2%) had non-operative management without embolization. There was no difference between cases and controls regarding incidence density of infections (44.1 (34.6-55.5)/1,000 person days vs 43.6 (37.7-50.2)/1,000 person days, incidence rate ratio=1 95% CI (0.77 to 1.3) p=0.94), type of infection, involved microorganisms, or severity (septic shock 12% vs 9.2%, p=0.6; acute respiratory distress syndrome 14% vs 9.2%, p=0.2).</p><p><strong>Conclusion: </strong>In the present study, AAST ≥III splenic trauma in severe trauma patients was not associated with an increased risk of infection during ICU stay.Level of evidence III.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 3","pages":"e001704"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001704","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Severe trauma can be responsible for a major systemic inflammatory response followed by post-traumatic immunosuppression. Immune imbalance promotes infections and increases mortality. This risk could be further increased in case of impaired splenic immune function due to splenic trauma. The objective of this study was to evaluate whether severe splenic trauma increased infectious complications in trauma patients during intensive care unit (ICU) stay.
Methods: This was an observational, bicentric, retrospective, case-control study including patients admitted for severe trauma from January 2011 to December 2020 in two level 1 trauma centers. Patients with American Association for the Surgery of Trauma (AAST) ≥III splenic trauma (case) were matched (1:3) with patients without splenic trauma (controls) according to age, sex, Injury Severity Score, initial Glasgow Coma Score, and Simplified Acute Physiology Score II. Demographic, trauma management, and infection data were collected. The primary endpoint was the incidence density of any infectious disease during ICU stay.
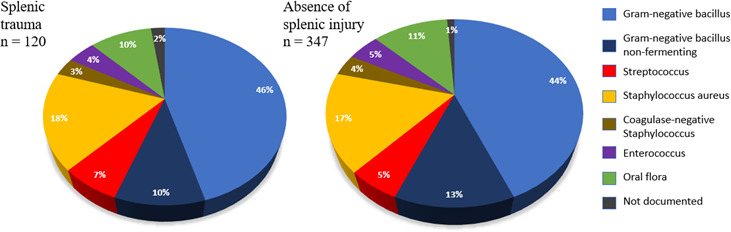
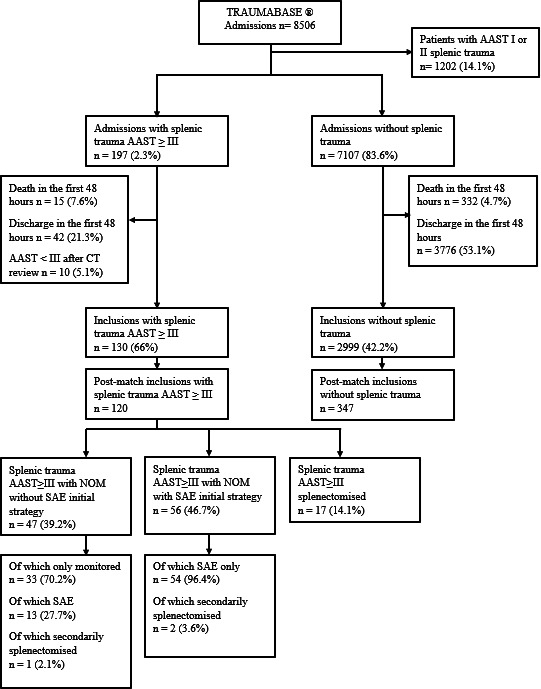
Results: Among 7,304 severe trauma patients, 130 patients with AAST ≥III splenic trauma were included. 10 patients could not be matched with controls. 17 patients (14.1%) underwent splenectomy, 56 patients (46.7%) had non-operative management with arterioembolization, and 47 (39.2%) had non-operative management without embolization. There was no difference between cases and controls regarding incidence density of infections (44.1 (34.6-55.5)/1,000 person days vs 43.6 (37.7-50.2)/1,000 person days, incidence rate ratio=1 95% CI (0.77 to 1.3) p=0.94), type of infection, involved microorganisms, or severity (septic shock 12% vs 9.2%, p=0.6; acute respiratory distress syndrome 14% vs 9.2%, p=0.2).
Conclusion: In the present study, AAST ≥III splenic trauma in severe trauma patients was not associated with an increased risk of infection during ICU stay.Level of evidence III.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


