Ahmed Abdelsamad, Mohammed Khaled Mohammed, Ibrahim Khalil, Zeyad M Wesh, Omar A Ahmed, Ahmed Elsherif, Jawad J F Alqedra, Khaled Ashraf Mohamed, Eslam Elmaghraby, Torsten Herzog, Florian Gebauer
{"title":"Continuous vs. interrupted suturing in hepaticojejunostomy: a comprehensive systematic review and meta-analysis.","authors":"Ahmed Abdelsamad, Mohammed Khaled Mohammed, Ibrahim Khalil, Zeyad M Wesh, Omar A Ahmed, Ahmed Elsherif, Jawad J F Alqedra, Khaled Ashraf Mohamed, Eslam Elmaghraby, Torsten Herzog, Florian Gebauer","doi":"10.1007/s00423-025-03756-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepaticojejunostomy (HJ) is a crucial reconstructive step in upper gastrointestinal (UGI), pancreaticoduodenectomy (PD), and Hepaticobiliarypancreatic (HBP) surgeries. The optimal suturing technique remains debated, with conflicting evidence regarding operative efficiency, costs, and complications. This meta-analysis compares continuous and interrupted suturing to provide evidence-based recommendations.</p><p><strong>Methods: </strong>A systematic review and meta-analysis were conducted using PubMed, Embase, and Cochrane Library. Primary outcomes were anastomotic time and costs, while secondary outcomes included bile leakage, anastomotic stricture, morbidity, cholangitis, hospital stay, and re-exploration rates. A random or fixed-effects model was applied based on heterogeneity. We included randomized controlled trials and non-randomized cohort studies. The risk of bias was assessed using the Cochrane ROB 2 tool, Newcastle-Ottawa Scale (NOS), and MINORS instrument as appropriate. Additionally, the quality of evidence for each outcome was evaluated using the GRADE approach. Sensitivity analyses were performed using the leave-one-out method.</p><p><strong>Results: </strong>Seven studies (1,159 patients) were included (continuous: 388, interrupted: 771). Continuous suturing significantly reduced anastomotic time (MD = -13.06 min, 95% CI: -17.37 to -8.75, P < 0.001) and costs (SMD = -4.89, 95% CI: -6.10 to -3.67, P < 0.001). However, no significant differences were observed in bile leakage, anastomotic stricture, morbidity, cholangitis, hospital stay, or re-exploration rates (P > 0.05). Sensitivity analyses confirmed these findings.</p><p><strong>Conclusion: </strong>Continuous suturing reduces anastomotic time by ~ 13 min and costs by ~ $90 without increasing complications. While these differences may be statistically significant, their clinical relevance can vary depending on the surgical context. Surgical choice should consider surgeon expertise, institutional protocols, and patient factors. Further randomized controlled trials are necessary to validate these findings.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"214"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227507/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03756-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hepaticojejunostomy (HJ) is a crucial reconstructive step in upper gastrointestinal (UGI), pancreaticoduodenectomy (PD), and Hepaticobiliarypancreatic (HBP) surgeries. The optimal suturing technique remains debated, with conflicting evidence regarding operative efficiency, costs, and complications. This meta-analysis compares continuous and interrupted suturing to provide evidence-based recommendations.
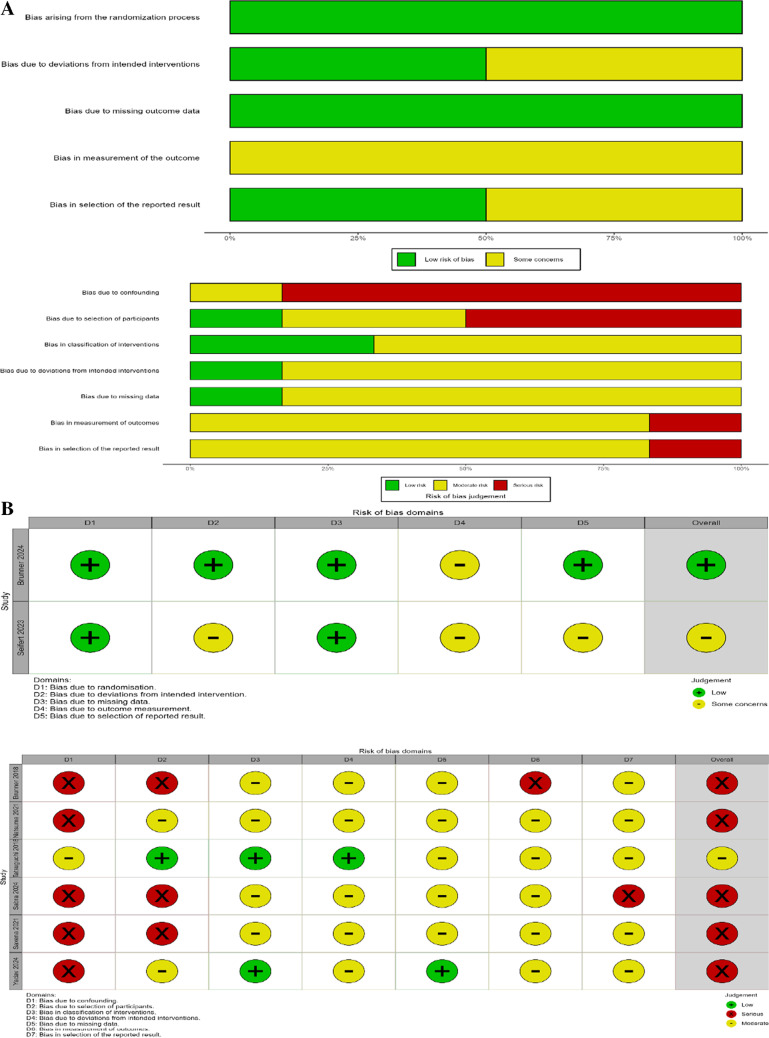
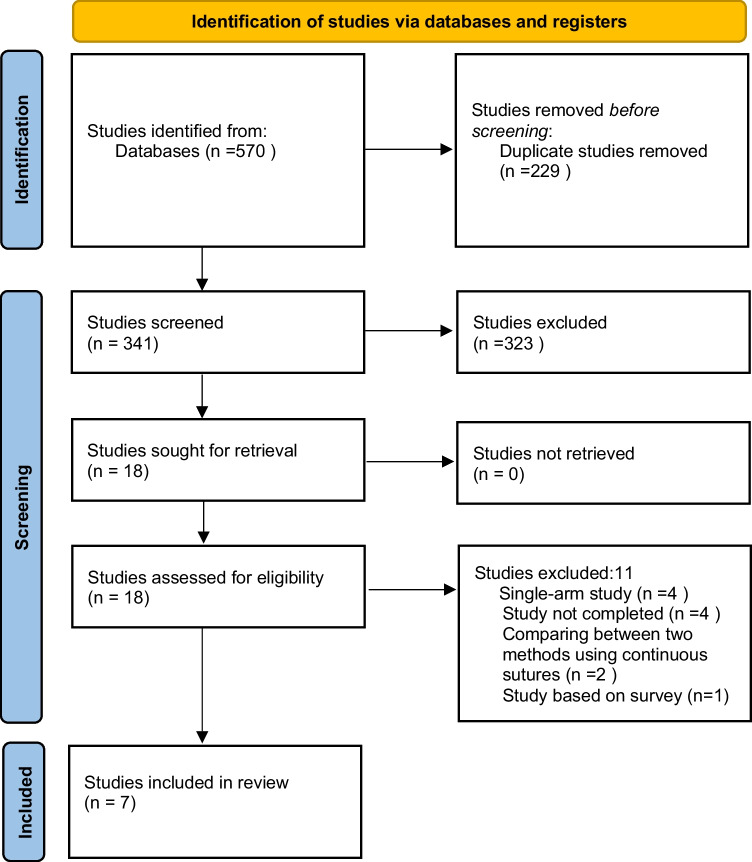
Methods: A systematic review and meta-analysis were conducted using PubMed, Embase, and Cochrane Library. Primary outcomes were anastomotic time and costs, while secondary outcomes included bile leakage, anastomotic stricture, morbidity, cholangitis, hospital stay, and re-exploration rates. A random or fixed-effects model was applied based on heterogeneity. We included randomized controlled trials and non-randomized cohort studies. The risk of bias was assessed using the Cochrane ROB 2 tool, Newcastle-Ottawa Scale (NOS), and MINORS instrument as appropriate. Additionally, the quality of evidence for each outcome was evaluated using the GRADE approach. Sensitivity analyses were performed using the leave-one-out method.
Results: Seven studies (1,159 patients) were included (continuous: 388, interrupted: 771). Continuous suturing significantly reduced anastomotic time (MD = -13.06 min, 95% CI: -17.37 to -8.75, P < 0.001) and costs (SMD = -4.89, 95% CI: -6.10 to -3.67, P < 0.001). However, no significant differences were observed in bile leakage, anastomotic stricture, morbidity, cholangitis, hospital stay, or re-exploration rates (P > 0.05). Sensitivity analyses confirmed these findings.
Conclusion: Continuous suturing reduces anastomotic time by ~ 13 min and costs by ~ $90 without increasing complications. While these differences may be statistically significant, their clinical relevance can vary depending on the surgical context. Surgical choice should consider surgeon expertise, institutional protocols, and patient factors. Further randomized controlled trials are necessary to validate these findings.
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


