Thibault Laban, Fredéric Pigneur, Constance Guillaud, Marie Agnès Dragon Durey, Houcine Hamidi, Caroline Pilon, Marc Michel, Nizar Joher, Philippe Grimbert, Hamza Sakhi, Antoine Morel, Marie Matignon
{"title":"Case Report: Failure of eculizumab to block complement to prevent relapse of anti-phospholipid syndrome in kidney transplant recipient.","authors":"Thibault Laban, Fredéric Pigneur, Constance Guillaud, Marie Agnès Dragon Durey, Houcine Hamidi, Caroline Pilon, Marc Michel, Nizar Joher, Philippe Grimbert, Hamza Sakhi, Antoine Morel, Marie Matignon","doi":"10.3389/fneph.2025.1572641","DOIUrl":null,"url":null,"abstract":"<p><p>Catastrophic antiphospholipid syndrome (CAPS) leads to organ dysfunction due to thrombotic microangiopathy (TMA). Complement may play a role in CAPS, and its blockade could prevent antiphospholipid syndrome (APS) complications after kidney transplantation (KT). Here, we report a case of APS recurrence after KT in a 38-year-old woman with early acute cortical kidney allograft necrosis despite preventive eculizumab treatment, probably because of insufficient complement blockade. The patient had recurrent but controlled CAPS for years with renal dysfunction, leading to preemptive KT. Anticoagulation and eculizumab were administered to prevent thrombosis and TMA after KT. She developed acute kidney injury (AKI) with incomplete biological TMA. Imaging revealed cortical necrosis in the renal allograft. In the absence of donor-specific anti-HLA antibodies, we concluded a relapse. Additional doses of eculizumab and plasma exchange allowed the normalization of biological tests and improvement of kidney allograft function. A retrospective complement analysis showed an incomplete blockade at the time of AKI. One year after KT, the renal allograft function was impaired. This suggests that inadequate complement blockade leads to a relapse of APS in the renal allograft with cortical necrosis and dysfunction. Our case highlights the importance of monitoring complement activity and adjusting the dose of eculizumab or ravulizumab.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"5 ","pages":"1572641"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12213432/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2025.1572641","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
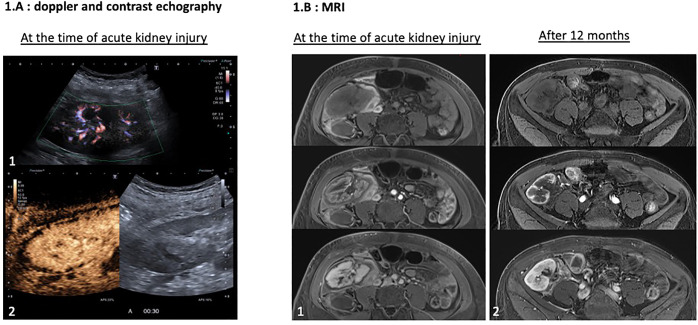
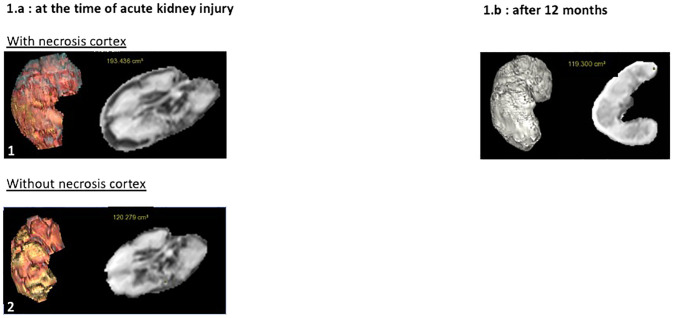
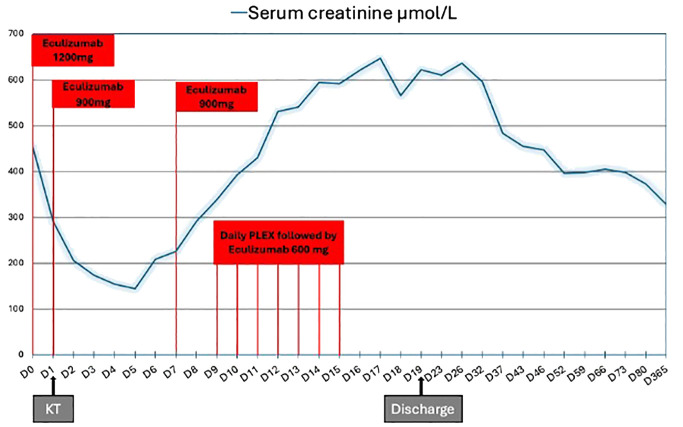
Catastrophic antiphospholipid syndrome (CAPS) leads to organ dysfunction due to thrombotic microangiopathy (TMA). Complement may play a role in CAPS, and its blockade could prevent antiphospholipid syndrome (APS) complications after kidney transplantation (KT). Here, we report a case of APS recurrence after KT in a 38-year-old woman with early acute cortical kidney allograft necrosis despite preventive eculizumab treatment, probably because of insufficient complement blockade. The patient had recurrent but controlled CAPS for years with renal dysfunction, leading to preemptive KT. Anticoagulation and eculizumab were administered to prevent thrombosis and TMA after KT. She developed acute kidney injury (AKI) with incomplete biological TMA. Imaging revealed cortical necrosis in the renal allograft. In the absence of donor-specific anti-HLA antibodies, we concluded a relapse. Additional doses of eculizumab and plasma exchange allowed the normalization of biological tests and improvement of kidney allograft function. A retrospective complement analysis showed an incomplete blockade at the time of AKI. One year after KT, the renal allograft function was impaired. This suggests that inadequate complement blockade leads to a relapse of APS in the renal allograft with cortical necrosis and dysfunction. Our case highlights the importance of monitoring complement activity and adjusting the dose of eculizumab or ravulizumab.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


