{"title":"End-of-life dignity in Home Hospice: Insights from staff members' narratives.","authors":"Gila Yakov, Gabriela Spector-Mersel, Inbal Halevi Hochwald","doi":"10.1177/26323524251349845","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dignity is a cornerstone of end-of-life (EoL) care, particularly in Home Hospice (HH) settings, where most patients wish to spend their final days. Despite HH staff's crucial role in preserving EoL dignity and their unique challenges, their views of EoL dignity remain underexplored. Moreover, the limited research draws on declarative descriptions, failing to capture the dynamic nature of EoL dignity as embedded in daily practice.</p><p><strong>Objectives: </strong>To address these gaps, we aimed to identify EoL dignity values and strategies embedded in HH staff's narratives on (in)dignity in their daily practice, that is, <i>dignity-in-action.</i></p><p><strong>Design: </strong>Qualitative research using narrative methodology.</p><p><strong>Methods: </strong>Drawing on the narrative research paradigm, 17 multidisciplinary HH staff members recounted cases of dignity or indignity in HH. An inductive, holistic content analysis of 32 narratives identified 48 endpoints illustrating (in)dignity incidents. These endpoints were analyzed to determine dignity values and the strategies used to uphold them. Finally, the endpoints were categorized by dignity values, strategies, and relations-who provided (in)dignity to whom.</p><p><strong>Results: </strong>The narratives presented HH staff as primary dignity providers, often identifying family members as sources of dignity violations. Dignity was framed around two core values, each upheld by three strategies. <i>Autonomy</i> was maintained by respecting patients' and families' preferences regarding care, staff-patient relationships, and coping strategies. <i>Individuality</i> was upheld by acknowledging and respecting the person beyond their patient status, honoring patients' and families' unique identities, and acknowledging and respecting patients' body image.</p><p><strong>Conclusion: </strong>HH care presents unique challenges in preserving EoL dignity but also offers opportunities for dignity-centered care. Respecting patients' and families' autonomy and individuality through targeted strategies can enhance dignified care. These insights underscore the need to embed dignity-preserving strategies into HH protocols and promote reflective training to heighten staff awareness of dignity violations while reinforcing their strengths in upholding patient and family dignity.</p>","PeriodicalId":36693,"journal":{"name":"Palliative Care and Social Practice","volume":"19 ","pages":"26323524251349845"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214316/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care and Social Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26323524251349845","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Dignity is a cornerstone of end-of-life (EoL) care, particularly in Home Hospice (HH) settings, where most patients wish to spend their final days. Despite HH staff's crucial role in preserving EoL dignity and their unique challenges, their views of EoL dignity remain underexplored. Moreover, the limited research draws on declarative descriptions, failing to capture the dynamic nature of EoL dignity as embedded in daily practice.
Objectives: To address these gaps, we aimed to identify EoL dignity values and strategies embedded in HH staff's narratives on (in)dignity in their daily practice, that is, dignity-in-action.
Design: Qualitative research using narrative methodology.
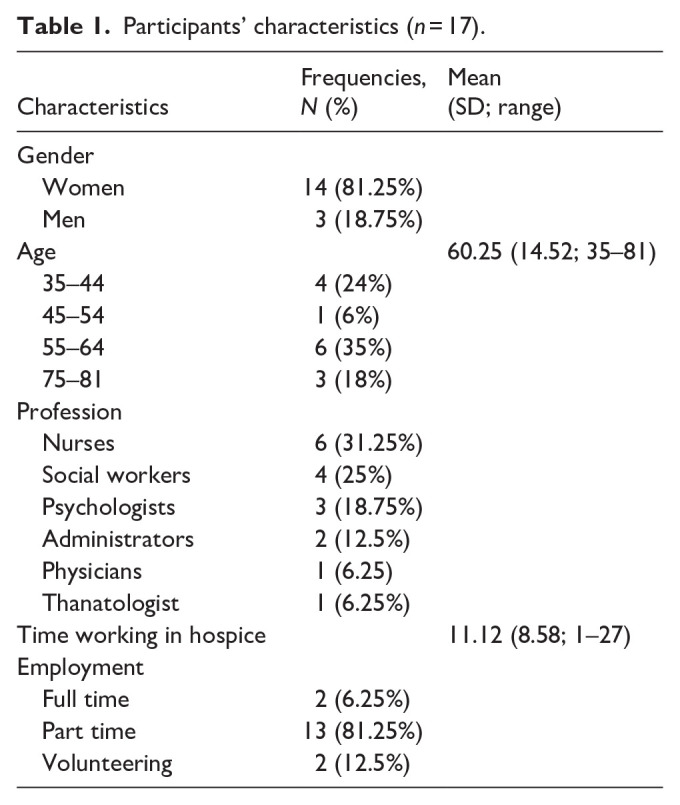
Methods: Drawing on the narrative research paradigm, 17 multidisciplinary HH staff members recounted cases of dignity or indignity in HH. An inductive, holistic content analysis of 32 narratives identified 48 endpoints illustrating (in)dignity incidents. These endpoints were analyzed to determine dignity values and the strategies used to uphold them. Finally, the endpoints were categorized by dignity values, strategies, and relations-who provided (in)dignity to whom.
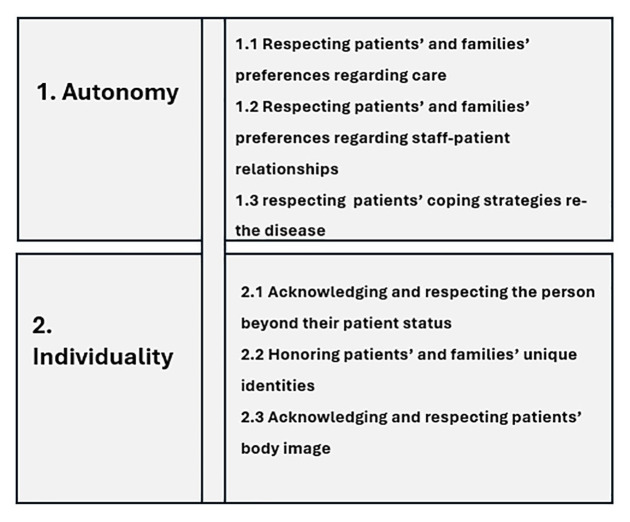
Results: The narratives presented HH staff as primary dignity providers, often identifying family members as sources of dignity violations. Dignity was framed around two core values, each upheld by three strategies. Autonomy was maintained by respecting patients' and families' preferences regarding care, staff-patient relationships, and coping strategies. Individuality was upheld by acknowledging and respecting the person beyond their patient status, honoring patients' and families' unique identities, and acknowledging and respecting patients' body image.
Conclusion: HH care presents unique challenges in preserving EoL dignity but also offers opportunities for dignity-centered care. Respecting patients' and families' autonomy and individuality through targeted strategies can enhance dignified care. These insights underscore the need to embed dignity-preserving strategies into HH protocols and promote reflective training to heighten staff awareness of dignity violations while reinforcing their strengths in upholding patient and family dignity.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


