Comparison between short-course and long-course antimicrobial treatments for acute cholangitis with gram-positive coccus bacteremia after endoscopic retrograde cholangiopancreatography.
{"title":"Comparison between short-course and long-course antimicrobial treatments for acute cholangitis with gram-positive coccus bacteremia after endoscopic retrograde cholangiopancreatography.","authors":"Yuntae Kim, Kazuhiro Ishikawa, Kenji Nakamura, Hikaru Ikusaka, Ryohsuke Yokosuka, Tomohiro Yamazaki, Yuichiro Suzuki, Shuhei Okuyama, Koichi Takagi, Katsuyuki Fukuda","doi":"10.4254/wjh.v17.i6.108100","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal duration of antimicrobial treatment for acute cholangitis complicated by gram-positive coccus (GPC) bacteremia remains unclear. The Tokyo Guidelines 2018 recommended 14 days of antimicrobial treatment following adequate source control measures; however, evidence supporting this recommendation is limited, and deviations from real-world practice are often observed.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of shorter antimicrobial treatments for acute cholangitis complicated by GPC bacteremia.</p><p><strong>Methods: </strong>Adult patients with acute cholangitis complicated by GPC bacteremia who underwent endoscopic retrograde cholangiopancreatography between July 2003 and December 2023 were included. Patients were categorized into two groups based on the duration of effective antimicrobial treatment: (1) Short-course treatment (SCT) (< 14 days); and (2) Long-course treatment (LCT) (≥ 14 days). The outcomes assessed included mortality, recurrence, reinfection with the same organism related to the cholangitis, and length of hospital stay.</p><p><strong>Results: </strong>A total of 44 patients were included in the study: (1) 19 patients in the SCT group; and (2) 25 patients in the LCT group. The median duration of antimicrobial treatment was 9 days [interquartile range (IQR): 2.5-11.0 days] and 16 days (IQR: 15.0-19.0 days) in the SCT and LCT groups, respectively, with a statistically significant difference (<i>P</i> < 0.05). No significant differences were observed in 30-day mortality, cholangitis recurrence, or reinfection with the same organisms within 3 months. However, the length of hospital stay was shorter in the SCT group (median: 12.0 days <i>vs</i> 14.0 days, <i>P</i> = 0.092).</p><p><strong>Conclusion: </strong>For acute cholangitis complicated by GPC bacteremia, shorter antimicrobial treatment may be a viable option following appropriate biliary drainage. Further studies with larger sample sizes are warranted.</p>","PeriodicalId":23687,"journal":{"name":"World Journal of Hepatology","volume":"17 6","pages":"108100"},"PeriodicalIF":2.5000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12210164/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4254/wjh.v17.i6.108100","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal duration of antimicrobial treatment for acute cholangitis complicated by gram-positive coccus (GPC) bacteremia remains unclear. The Tokyo Guidelines 2018 recommended 14 days of antimicrobial treatment following adequate source control measures; however, evidence supporting this recommendation is limited, and deviations from real-world practice are often observed.
Aim: To evaluate the efficacy and safety of shorter antimicrobial treatments for acute cholangitis complicated by GPC bacteremia.
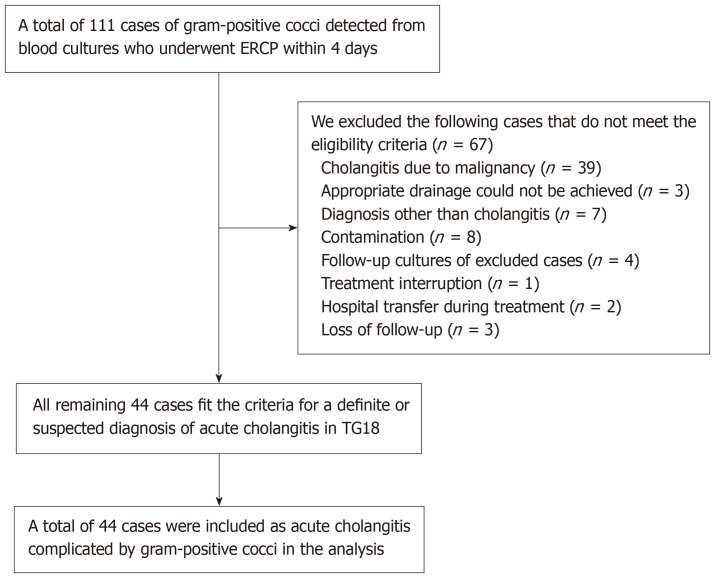
Methods: Adult patients with acute cholangitis complicated by GPC bacteremia who underwent endoscopic retrograde cholangiopancreatography between July 2003 and December 2023 were included. Patients were categorized into two groups based on the duration of effective antimicrobial treatment: (1) Short-course treatment (SCT) (< 14 days); and (2) Long-course treatment (LCT) (≥ 14 days). The outcomes assessed included mortality, recurrence, reinfection with the same organism related to the cholangitis, and length of hospital stay.
Results: A total of 44 patients were included in the study: (1) 19 patients in the SCT group; and (2) 25 patients in the LCT group. The median duration of antimicrobial treatment was 9 days [interquartile range (IQR): 2.5-11.0 days] and 16 days (IQR: 15.0-19.0 days) in the SCT and LCT groups, respectively, with a statistically significant difference (P < 0.05). No significant differences were observed in 30-day mortality, cholangitis recurrence, or reinfection with the same organisms within 3 months. However, the length of hospital stay was shorter in the SCT group (median: 12.0 days vs 14.0 days, P = 0.092).
Conclusion: For acute cholangitis complicated by GPC bacteremia, shorter antimicrobial treatment may be a viable option following appropriate biliary drainage. Further studies with larger sample sizes are warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


