Rifampicin Exposure in Tuberculosis Patients with Comorbidities in Sub-Saharan Africa: Prioritising Populations for Treatment-A Systematic Review and Meta-analysis.
Bibie Said, Yuan Pétermann, Patrick Howlett, Monia Guidi, Yann Thoma, Violet Dismas Kajogoo, Margaretha Sariko, Scott K Heysell, Jan-Willem Alffenaar, Emmanuel Mpolya, Stellah Mpagama
{"title":"Rifampicin Exposure in Tuberculosis Patients with Comorbidities in Sub-Saharan Africa: Prioritising Populations for Treatment-A Systematic Review and Meta-analysis.","authors":"Bibie Said, Yuan Pétermann, Patrick Howlett, Monia Guidi, Yann Thoma, Violet Dismas Kajogoo, Margaretha Sariko, Scott K Heysell, Jan-Willem Alffenaar, Emmanuel Mpolya, Stellah Mpagama","doi":"10.1007/s40262-025-01537-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Emerging evidence suggests that comorbidities like human immunodeficiency virus (HIV) infection, diabetes mellitus (DM), and malnutrition in tuberculosis (TB) patients can alter drug concentrations, thereby affecting the treatment outcomes. For these populations, personalised strategies such as therapeutic drug monitoring (TDM) may be essential. We investigated the variations of drug levels within comorbid populations and analysed the differences in patterns observed between sub-Saharan Africa (SSA) and non-SSA regions.</p><p><strong>Methods: </strong>We performed a systematic review and meta-analysis of rifampicin drug pharmacokinetics (PK) through searches of major databases from 1980 to December 2023. A random-effects meta-analysis model using R-studio version 4.3.2 was conducted to estimate pooled serum rifampicin exposure (area under the concentration-time curve [AUC], and peak maximum concentration [C<sub>max</sub>]) between patients with TB-HIV infection, and TB-DM.</p><p><strong>Results: </strong>From 3300 articles screened, 24 studies met inclusion criteria, contributing 33 comorbidity subgroups for meta-analysis. In SSA, 14 subgroups assessed rifampicin PK in TB-HIV, 1 in TB-DM, and none in TB-malnutrition. The pooled mean C<sub>max</sub> was below the recommended range (8-24 mg/L) for all subgroups. For TB-HIV, the pooled C<sub>max</sub> was 5.59 mg/L, 95% CI (4.59-6.59), I<sup>2</sup> = 97% for SSA populations and 5.59 mg/L, 95% CI (3.65; 6.59) for non-SSA populations. The C<sub>max</sub> for TB-DM in SSA (9.60 ± 4.4 mg/L) exceeded non-SSA (4.27 mg/L, 95% CI [2.77-5.76]). The lowest AUC was in TB-HIV (SSA, 29.09 mg/L h, 95% CI [21.06; 37.13, I<sup>2</sup> = 91%]). High variability and heterogeneity (I<sup>2</sup> >90%) were observed, with most studies (20/23) showing low bias.</p><p><strong>Conclusion: </strong>Our results emphasise the need for individualised dosing and targeted TDM implementation among TB-HIV and TB-DM populations on rifampicin in SSA. Although all populations exhibited low C<sub>max</sub> levels, TB-HIV populations may be prioritised as AUC levels were lowest. In clinical settings in SSA, C<sub>max</sub>-based TDM is more practical, but AUC can be used in treatment where feasible.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"1149-1163"},"PeriodicalIF":4.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12263804/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01537-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: Emerging evidence suggests that comorbidities like human immunodeficiency virus (HIV) infection, diabetes mellitus (DM), and malnutrition in tuberculosis (TB) patients can alter drug concentrations, thereby affecting the treatment outcomes. For these populations, personalised strategies such as therapeutic drug monitoring (TDM) may be essential. We investigated the variations of drug levels within comorbid populations and analysed the differences in patterns observed between sub-Saharan Africa (SSA) and non-SSA regions.
Methods: We performed a systematic review and meta-analysis of rifampicin drug pharmacokinetics (PK) through searches of major databases from 1980 to December 2023. A random-effects meta-analysis model using R-studio version 4.3.2 was conducted to estimate pooled serum rifampicin exposure (area under the concentration-time curve [AUC], and peak maximum concentration [Cmax]) between patients with TB-HIV infection, and TB-DM.
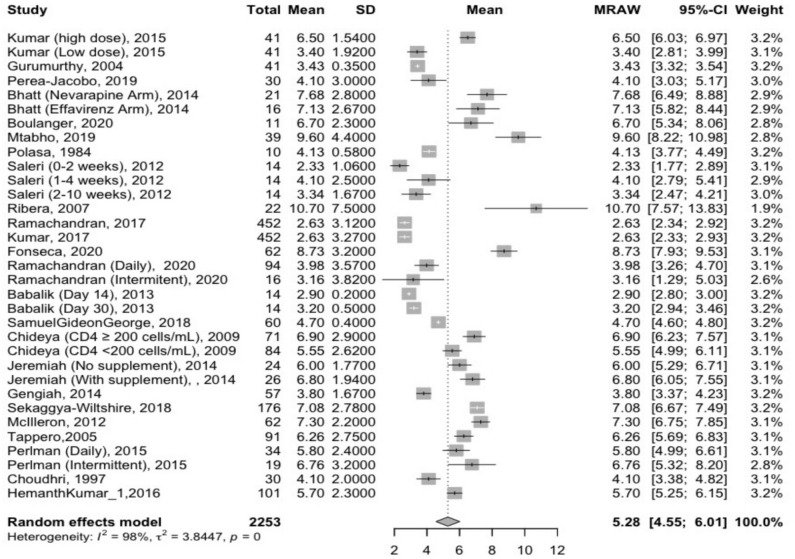
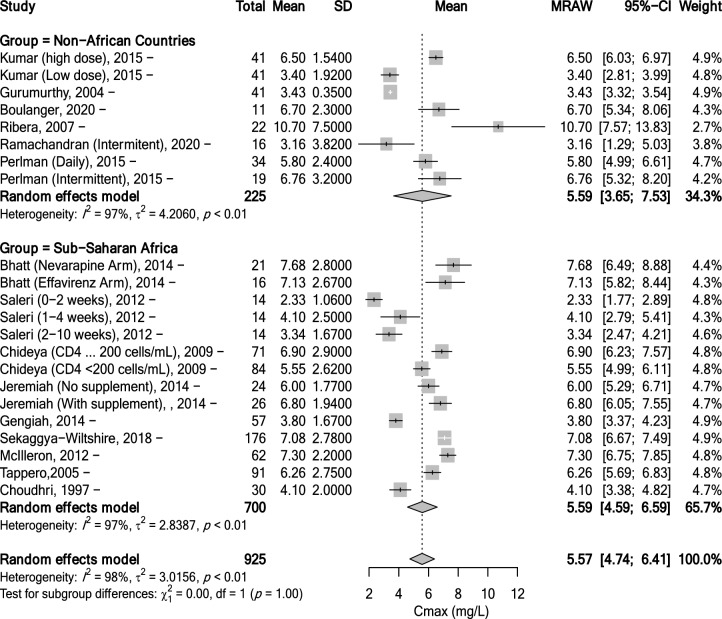
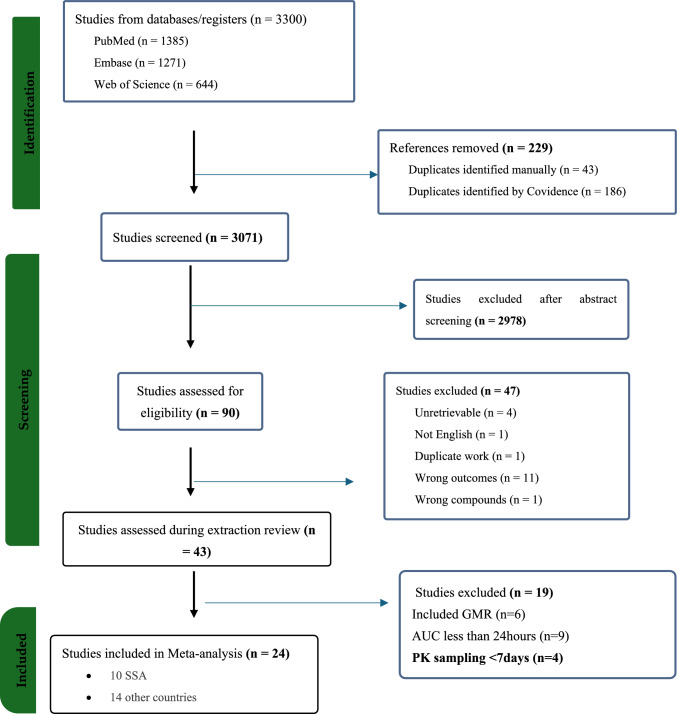
Results: From 3300 articles screened, 24 studies met inclusion criteria, contributing 33 comorbidity subgroups for meta-analysis. In SSA, 14 subgroups assessed rifampicin PK in TB-HIV, 1 in TB-DM, and none in TB-malnutrition. The pooled mean Cmax was below the recommended range (8-24 mg/L) for all subgroups. For TB-HIV, the pooled Cmax was 5.59 mg/L, 95% CI (4.59-6.59), I2 = 97% for SSA populations and 5.59 mg/L, 95% CI (3.65; 6.59) for non-SSA populations. The Cmax for TB-DM in SSA (9.60 ± 4.4 mg/L) exceeded non-SSA (4.27 mg/L, 95% CI [2.77-5.76]). The lowest AUC was in TB-HIV (SSA, 29.09 mg/L h, 95% CI [21.06; 37.13, I2 = 91%]). High variability and heterogeneity (I2 >90%) were observed, with most studies (20/23) showing low bias.
Conclusion: Our results emphasise the need for individualised dosing and targeted TDM implementation among TB-HIV and TB-DM populations on rifampicin in SSA. Although all populations exhibited low Cmax levels, TB-HIV populations may be prioritised as AUC levels were lowest. In clinical settings in SSA, Cmax-based TDM is more practical, but AUC can be used in treatment where feasible.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


