Jennifer Herrera-Mullar, Carolyn Horton, Amybeth Weaver, Meghan Towne, Jennifer M Huang, Grace E VanNoy, Steven M Harrison, Bess Wayburn
{"title":"Understanding how gene-disease relationships can impact clinical utility: adaptations and challenges in hereditary cancer testing.","authors":"Jennifer Herrera-Mullar, Carolyn Horton, Amybeth Weaver, Meghan Towne, Jennifer M Huang, Grace E VanNoy, Steven M Harrison, Bess Wayburn","doi":"10.1186/s13073-025-01499-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Defining gene-disease relationships (GDRs) influences the clinical utility of hereditary cancer predisposition (HCP) multigene panel testing (MGPT) results, as variant classification relies directly on gene-disease characterization. GDR characterization for HCP is challenging due to disease prevalence, incomplete penetrance, and heterogeneity. There is insufficient data showing how gene-disease validity (GDV) scores of HCP genes affect variant classification and how GDV scores change over time. Though these issues determine the results of HCP-MGPT, their impact on short- and long-term clinical utility has not been explored in-depth.</p><p><strong>Methods: </strong>Using an evidence-based GDV framework, genes were classified into five standardized GDV categories at the time of panel addition. We curated changes in GDV scores and classifications for HCP-MGPT over 7 years. The corresponding impact on the frequency of positive and variant of uncertain significance (VUS) results was evaluated by GDV score.</p><p><strong>Results: </strong>Positive results were most common in Definitive evidence genes (31.5%), with none in Limited evidence genes (0%). Genes with Definitive GDRs (n = 42) remained Definitive, while most genes with Strong (6/10, 60%) and Moderate (19/24, 80%) GDRs changed categories, 8 (23.5%) of which received a clinically significant GDR downgrade. GDRs associated with low-moderate risk of breast cancer were significantly more likely to be downgraded compared to GDRs associated with rarer, high-penetrance specific phenotypes (p < 0.0001). Downgrades for all GDRs were due to new published data and updates to the GDV framework (77%, 10/13), with 23% (3/13) due to framework updates alone. Including Limited evidence genes on MGPT increased the VUS frequency by 13.7% percentage points.</p><p><strong>Conclusions: </strong>Positive and VUS results varied by GDV category, and Limited evidence genes did not contribute to diagnostic yield. No Limited evidence genes in the category for ≥ 3 years (n = 8) were upgraded, indicating that including these genes on HCP-MGPT provides limited long-term clinical utility. Our data highlight that GDV assessment for HCP requires robust evidence and must account for variable disease penetrance and elevated prevalence in the population. Balancing the availability of a comprehensive gene menu and transparency surrounding clinical utility of novel genes will maximize identification of high-risk patients while reducing the risk of misdiagnosis through clinical false-positive results.</p>","PeriodicalId":12645,"journal":{"name":"Genome Medicine","volume":"17 1","pages":"73"},"PeriodicalIF":10.4000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12220650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Genome Medicine","FirstCategoryId":"99","ListUrlMain":"https://doi.org/10.1186/s13073-025-01499-5","RegionNum":1,"RegionCategory":"生物学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Defining gene-disease relationships (GDRs) influences the clinical utility of hereditary cancer predisposition (HCP) multigene panel testing (MGPT) results, as variant classification relies directly on gene-disease characterization. GDR characterization for HCP is challenging due to disease prevalence, incomplete penetrance, and heterogeneity. There is insufficient data showing how gene-disease validity (GDV) scores of HCP genes affect variant classification and how GDV scores change over time. Though these issues determine the results of HCP-MGPT, their impact on short- and long-term clinical utility has not been explored in-depth.
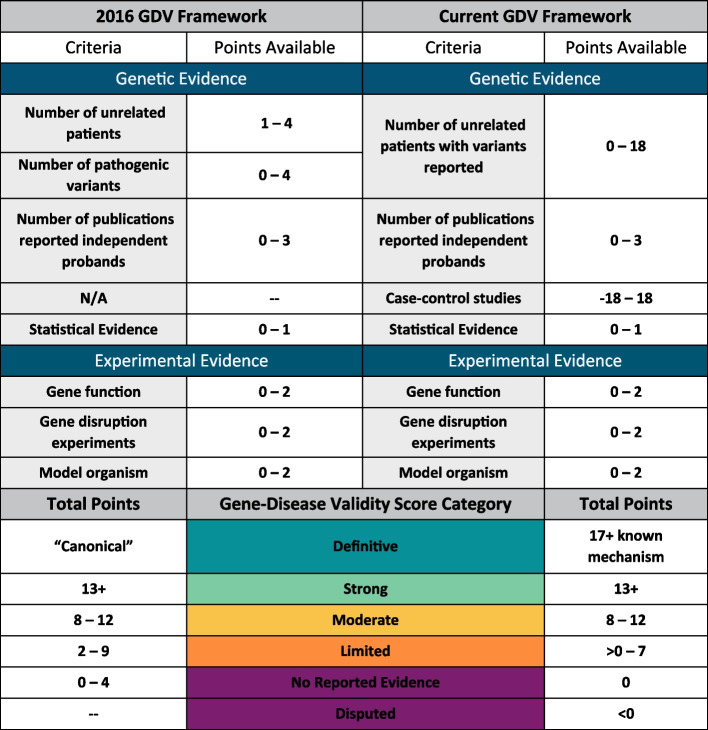
Methods: Using an evidence-based GDV framework, genes were classified into five standardized GDV categories at the time of panel addition. We curated changes in GDV scores and classifications for HCP-MGPT over 7 years. The corresponding impact on the frequency of positive and variant of uncertain significance (VUS) results was evaluated by GDV score.
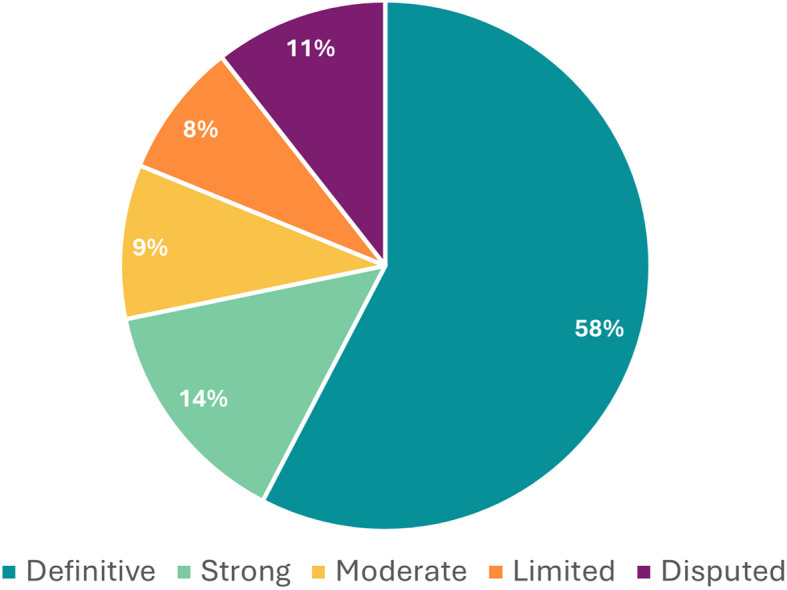
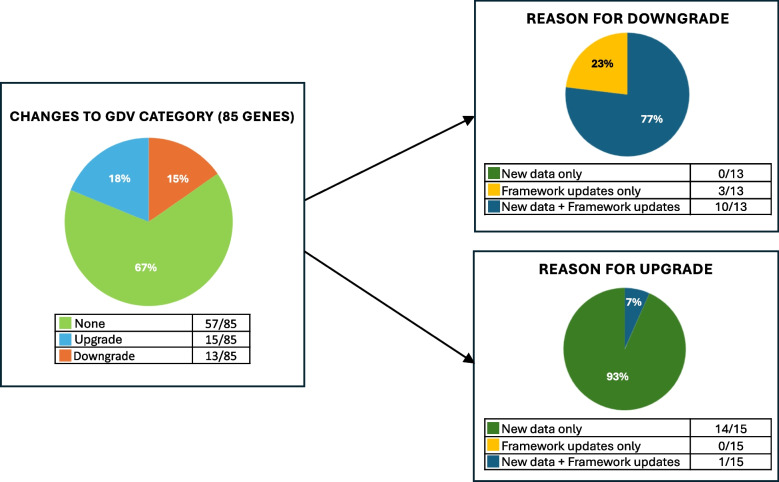
Results: Positive results were most common in Definitive evidence genes (31.5%), with none in Limited evidence genes (0%). Genes with Definitive GDRs (n = 42) remained Definitive, while most genes with Strong (6/10, 60%) and Moderate (19/24, 80%) GDRs changed categories, 8 (23.5%) of which received a clinically significant GDR downgrade. GDRs associated with low-moderate risk of breast cancer were significantly more likely to be downgraded compared to GDRs associated with rarer, high-penetrance specific phenotypes (p < 0.0001). Downgrades for all GDRs were due to new published data and updates to the GDV framework (77%, 10/13), with 23% (3/13) due to framework updates alone. Including Limited evidence genes on MGPT increased the VUS frequency by 13.7% percentage points.
Conclusions: Positive and VUS results varied by GDV category, and Limited evidence genes did not contribute to diagnostic yield. No Limited evidence genes in the category for ≥ 3 years (n = 8) were upgraded, indicating that including these genes on HCP-MGPT provides limited long-term clinical utility. Our data highlight that GDV assessment for HCP requires robust evidence and must account for variable disease penetrance and elevated prevalence in the population. Balancing the availability of a comprehensive gene menu and transparency surrounding clinical utility of novel genes will maximize identification of high-risk patients while reducing the risk of misdiagnosis through clinical false-positive results.
期刊介绍:
Genome Medicine is an open access journal that publishes outstanding research applying genetics, genomics, and multi-omics to understand, diagnose, and treat disease. Bridging basic science and clinical research, it covers areas such as cancer genomics, immuno-oncology, immunogenomics, infectious disease, microbiome, neurogenomics, systems medicine, clinical genomics, gene therapies, precision medicine, and clinical trials. The journal publishes original research, methods, software, and reviews to serve authors and promote broad interest and importance in the field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


